 RSS Feed
RSS Feed Twitter
Twitter


 Sunday, March 29, 2015
Sunday, March 29, 2015
 Unknown
Unknown
Chronic obstructive pulmonary disease (COPD) is estimated to affect 32 million persons in the United States and is the third leading cause of death in this country. Patients typically have symptoms of chronic bronchitis and emphysema, but the classic triad also includes asthma (see the image below).
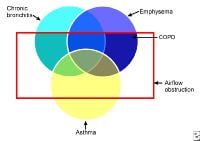 Venn diagram of chronic obstructive pulmonary disease (COPD). Chronic obstructive lung disease is a disorder in which subsets of patients may have dominant features of chronic bronchitis, emphysema, or asthma. The result is airflow obstruction that is not fully reversible.
Venn diagram of chronic obstructive pulmonary disease (COPD). Chronic obstructive lung disease is a disorder in which subsets of patients may have dominant features of chronic bronchitis, emphysema, or asthma. The result is airflow obstruction that is not fully reversible.
Chronic bronchitis is defined clinically as the presence of a chronic productive cough for 3 months during each of 2 consecutive years (other causes of cough being excluded). Emphysema is defined pathologically as an abnormal, permanent enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis.
Essential update: FDA approves olodaterol for COPD
The FDA has approved olodaterol (Striverdi Respimat), a long-acting beta-agonist, for the long-term, once-daily maintenance treatment of airflow obstruction in patients with COPD, including chronic bronchitis and/or emphysema. Approval was based on a study of 3104 patients in which olodaterol improved lung function compared with placebo.
Olodaterol should not be used as a rescue therapy for acute bronchospasm or in patients with acutely deteriorating COPD or with asthma. Potential serious side effects include paradoxical bronchospasm and cardiovascular effects.
Signs and symptoms
Patients typically present with a combination of signs and symptoms of chronic bronchitis, emphysema, and reactive airway disease. Symptoms include the following:
- Cough, usually worse in the mornings and productive of a small amount of colorless sputum
- Acute chest illness
- Breathlessness: The most significant symptom, but usually does not occur until the sixth decade of life
- Wheezing: May occur in some patients, particularly during exertion and exacerbations
The sensitivity of physical examination in detecting mild to moderate COPD is relatively poor, but physical signs are quite specific and sensitive for severe disease. Findings in severe disease include the following:
- Tachypnea and respiratory distress with simple activities
- Use of accessory respiratory muscles and paradoxical indrawing of lower intercostal spaces (Hoover sign)
- Cyanosis
- Elevated jugular venous pulse (JVP)
- Peripheral edema
Thoracic examination reveals the following:
- Hyperinflation (barrel chest)
- Wheezing – Frequently heard on forced and unforced expiration
- Diffusely decreased breath sounds
- Hyperresonance on percussion
- Prolonged expiration
- Coarse crackles beginning with inspiration in some cases
Certain characteristics allow differentiation between disease that is predominantly chronic bronchitis and that which is predominantly emphysema. Chronic bronchitis characteristics include the following:
- Patients may be obese
- Frequent cough and expectoration are typical
- Use of accessory muscles of respiration is common
- Coarse rhonchi and wheezing may be heard on auscultation
- Patients may have signs of right heart failure (ie, cor pulmonale), such as edema and cyanosis
Emphysema characteristics include the following:
- Patients may be very thin with a barrel chest
- Patients typically have little or no cough or expectoration
- Breathing may be assisted by pursed lips and use of accessory respiratory muscles; patients may adopt the tripod sitting position
- The chest may be hyperresonant, and wheezing may be heard
- Heart sounds are very distant
- Overall appearance is more like classic COPD exacerbation
Diagnosis
The formal diagnosis of COPD is made with spirometry; when the ratio of forced expiratory volume in 1 second over forced vital capacity (FEV1/FVC) is less than 70% of that predicted for a matched control, it is diagnostic for a significant obstructive defect. Criteria for assessing the severity of airflow obstruction (based on the percent predicted postbronchodilator FEV1) are as follows:
- Stage I (mild): FEV 1 80% or greater of predicted
- Stage II (moderate): FEV 1 50-79% of predicted
- Stage III (severe): FEV 1 30-49% of predicted
- Stage IV (very severe): FEV 1 less than 30% of predicted or FEV 1 less than 50% and chronic respiratory failure
Arterial blood gas (ABG) findings are as follows:
- ABGs provide the best clues as to acuteness and severity of disease exacerbation
- Patients with mild COPD have mild to moderate hypoxemia without hypercapnia
- As the disease progresses, hypoxemia worsens and hypercapnia may develop, with the latter commonly being observed as the FEV 1 falls below 1 L/s or 30% of the predicted value
- pH usually is near normal; a pH below 7.3 generally indicates acute respiratory compromise
- Chronic respiratory acidosis leads to compensatory metabolic alkalosis
In patients with emphysema, frontal and lateral chest radiographs reveal the following:
- Flattening of the diaphragm
- Increased retrosternal air space
- A long, narrow heart shadow
- Rapidly tapering vascular shadows accompanied by hyperlucency of the lungs
- Radiographs in patients with chronic bronchitis show increased bronchovascular markings and cardiomegaly
Advantages of high-resolution CT include the following:
- Greater sensitivity than standard chest radiography
- High specificity for diagnosing emphysema (outlined bullae are not always visible on a radiograph)
- May provide an adjunctive means of diagnosing various forms of COPD (eg, lower lobe disease may suggest alpha1-antitrypsin (AAT) deficiency
- May help the clinician determine whether surgical intervention would benefit the patient
Other tests are as follows:
- Hematocrit – Patients with polycythemia (hematocrit greater than 52% in men or 47% in women) should be evaluated for hypoxemia at rest, with exertion, or during sleep
- Serum potassium – Diuretics, beta-adrenergic agonists, and theophylline act to lower potassium levels
- Measure AAT in all patients younger than 40 years or in those with a family history of emphysema at an early age
- Sputum evaluation will show a transformation from mucoid in stable chronic bronchitis to purulent in acute exacerbations
- Pulse oximetry, combined with clinical observation, provides instant feedback on a patient's status
- Electrocardiography can help establish that hypoxia is not resulting in cardiac ischemia and that the underlying cause of respiratory difficulty is not cardiac in nature
- The distance walked in 6 minutes (6MWD) is a good predictor of all-cause and respiratory mortality in patients with moderate COPD [2, 3] ; patients with COPD who desaturate during the 6MWD have a higher mortality rate than do those who do not desaturate
- Two-dimensional echocardiography can screen for pulmonary hypertension
- Right-sided heart catheterization can confirm pulmonary artery hypertension and gauge the response to vasodilators
Management
Smoking cessation continues to be the most important therapeutic intervention for COPD. Risk factor reduction (eg, influenza vaccine) is appropriate for all stages of COPD. Approaches to management by stage include the following:
- Stage I (mild obstruction): Short-acting bronchodilator as needed
- Stage II (moderate obstruction): Short-acting bronchodilator as needed; long-acting bronchodilator(s); cardiopulmonary rehabilitation
- Stage III (severe obstruction): Short-acting bronchodilator as needed; long-acting bronchodilator(s); cardiopulmonary rehabilitation; inhaled glucocorticoids if repeated exacerbations
- Stage IV (very severe obstruction or moderate obstruction with evidence of chronic respiratory failure): Short-acting bronchodilator as needed; long-acting bronchodilator(s); cardiopulmonary rehabilitation; inhaled glucocorticoids if repeated exacerbation; long-term oxygen therapy (if criteria met); consider surgical options such as lung volume reduction surgery (LVRS) and lung transplantation
Agents used include the following:
- Short-acting beta 2 -agonist bronchodilators (eg, albuterol, metaproterenol, levalbuterol, pirbuterol)
- Long-acting beta 2 -agonist bronchodilators (eg, salmeterol, formoterol, arformoterol, indacaterol, vilanterol)
- Respiratory anticholinergics (eg, ipratropium, tiotropium, aclidinium)
- Xanthine derivatives (ie, theophylline)
- Phosphodiesterase-4 Inhibitors (ie, roflumilast)
- Inhaled corticosteroids (eg, fluticasone, budesonide)
- Oral corticosteroids (eg, prednisone)
- Beta 2 -agonist and anticholinergic combinations (eg, ipratropium and albuterol, umeclidinium bromide/vilanterol inhaled)
- Beta 2 -agonist and corticosteroid combinations (eg, budesonide/formoterol, fluticasone and salmeterol, vilanterol/fluticasone inhaled)
Pulmonary rehabilitation programs are typically multidisciplinary approaches that emphasize the following:
- Patient and family education
- Smoking cessation
- Medical management (including oxygen and immunization)
- Respiratory and chest physiotherapy
- Physical therapy with bronchopulmonary hygiene, exercise, and vocational rehabilitation
- Psychosocial support
Indications for admission for acute exacerbations include the following:
- Failure of outpatient treatment
- Marked increase in dyspnea
- Altered mental status
- Increase in hypoxemia or hypercapnia
- Inability to tolerate oral medications such as antibiotics or steroids
Background
Chronic obstructive pulmonary disease (COPD) is estimated to affect 32 million persons in the United States and is the third leading cause of death in this country. Patients typically have symptoms of chronic bronchitis and emphysema, but the classic triad also includes asthma (as seen in the image below). (See Clinical Presentation.)
Venn diagram of chronic obstructive pulmonary disease (COPD). Chronic obstructive lung disease is a disorder in which subsets of patients may have dominant features of chronic bronchitis, emphysema, or asthma. The result is airflow obstruction that is not fully reversible.
In Western Europe, Badham (1808) and Laennec (1827) made the classic descriptions of chronic bronchitis and emphysema in the early 19th century. A British medical textbook of the 1860s described the familiar clinical picture of chronic bronchitis as an advanced disease with repeated bronchial infections that ended in right-sided heart failure. Overall, this malady caused more than 5% of all deaths in the Middle Ages and earlier. The condition was most common among the poor; therefore, it was attributed to "bad" living.
Developments in the 20th century included the widespread use of spirometry (see Workup), recognition of airflow obstruction as a key factor in determining disability, and the improvement of pathologic methods to assess emphysema. Participants in the Ciba symposium of 1958 proposed definitions of chronic bronchitis and emphysema, incorporating the concept of airflow obstruction.
Chronic bronchitis is defined clinically as the presence of a chronic productive cough for 3 months during each of 2 consecutive years (other causes of cough being excluded). Emphysema, on the other hand, is defined pathologically as an abnormal, permanent enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis.
Airflow limitation in emphysema is due to loss of elastic recoil and decrease in airway tethering, whereas chronic bronchitis leads to narrowing of airway caliber and increase in airway resistance. Although some patients predominantly display signs of one of these diseases or the other, most fall somewhere in the middle of the spectrum between the 2 conditions.
Past definitions of COPD have been pessimistic at best, indicating that the disease process is irreversible and that therapy has little to offer. However, a more optimistic view has come to be widely accepted. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines define COPD as a disease state characterized by airflow limitation that is not fully reversible, is usually progressive, and is associated with an abnormal inflammatory response of the lungs to inhaled noxious particles or gases,[4] (See Clinical Presentation.)
This GOLD characterization represents a paradigm shift—it suggests that the disease is treatable and preventable. (For a guideline summary, see Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease.[5] ) (See Treatment and Management.)
Oral and inhaled medications are used for patients with stable COPD to reduce dyspnea, improve exercise tolerance, and prevent complications. Most of the medications used in COPD treatment are directed at the potentially reversible mechanisms of airflow limitation. (See Medication.)
Pathophysiology
Pathologic changes in chronic obstructive pulmonary disease (COPD) occur in the large (central) airways, the small (peripheral) bronchioles, and the lung parenchyma. Most cases of COPD are the result of exposure to noxious stimuli, most often cigarette smoke. The normal inflammatory response is amplified in persons prone to COPD development. The pathogenic mechanisms are not clear but are most likely diverse. Increased numbers of activated polymorphonuclear leukocytes and macrophages release elastases in a manner that cannot be counteracted effectively by antiproteases, resulting in lung destruction.
The primary offender has been found to be human leukocyte elastase, with synergistic roles suggested for proteinase-3 and macrophage-derived matrix metalloproteinases (MMPs), cysteine proteinases, and a plasminogen activator. Additionally, increased oxidative stress caused by free radicals in cigarette smoke, the oxidants released by phagocytes, and polymorphonuclear leukocytes all may lead to apoptosis or necrosis of exposed cells. Accelerated aging and autoimmune mechanisms have also been proposed as having roles in the pathogenesis of COPD.
Cigarette smoke causes neutrophil influx, which is required for the secretion of MMPs; this suggests, therefore, that neutrophils and macrophages are required for the development of emphysema.
Studies have also shown that in addition to macrophages, T lymphocytes, particularly CD8+, play an important role in the pathogenesis of smoking-induced airflow limitation.
To support the inflammation hypothesis further, a stepwise increase in alveolar inflammation has been found in surgical specimens from patients without COPD versus patients with mild or severe emphysema. Indeed, mounting evidence supports the concept that dysregulation of apoptosis and defective clearance of apoptotic cells by macrophages play a prominent role in airway inflammation, particularly in emphysema.Azithromycin (Zithromax) has been shown to improve this macrophage clearance function, providing a possible future treatment modality.
In patients with stable COPD without known cardiovascular disease, there is a high prevalence of microalbuminuria, which is associated with hypoxemia independent of other risk factors.
Chronic bronchitis
Mucous gland hyperplasia (as seen in the images below) is the histologic hallmark of chronic bronchitis. Airway structural changes include atrophy, focal squamous metaplasia, ciliary abnormalities, variable amounts of airway smooth muscle hyperplasia, inflammation, and bronchial wall thickening.
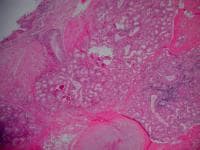 Histopathology of chronic bronchitis showing hyperplasia of mucous glands and infiltration of the airway wall with inflammatory cells.
Histopathology of chronic bronchitis showing hyperplasia of mucous glands and infiltration of the airway wall with inflammatory cells.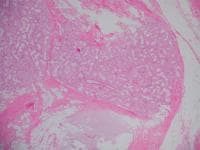 Histopathology of chronic bronchitis showing hyperplasia of mucous glands and infiltration of the airway wall with inflammatory cells (high-powered view).
Histopathology of chronic bronchitis showing hyperplasia of mucous glands and infiltration of the airway wall with inflammatory cells (high-powered view).
Damage to the endothelium impairs the mucociliary response that clears bacteria and mucus. Inflammation and secretions provide the obstructive component of chronic bronchitis. Neutrophilia develops in the airway lumen, and neutrophilic infiltrates accumulate in the submucosa. The respiratory bronchioles display a mononuclear inflammatory process, lumen occlusion by mucus plugging, goblet cell metaplasia, smooth muscle hyperplasia, and distortion due to fibrosis. These changes, combined with loss of supporting alveolar attachments, cause airflow limitation by allowing airway walls to deform and narrow the airway lumen.
In contrast to emphysema, chronic bronchitis is associated with a relatively undamaged pulmonary capillary bed. The body responds by decreasing ventilation and increasing cardiac output. This V/Q mismatch results in rapid circulation in a poorly ventilated lung, leading to hypoxemia and polycythemia. Eventually, hypercapnia and respiratory acidosis develop, leading to pulmonary artery vasoconstriction and cor pulmonale. With the ensuing hypoxemia, polycythemia, and increased CO2 retention, these patients have signs of right heart failure and are known as "blue bloaters."
Emphysema
Emphysema is a pathologic diagnosis defined by permanent enlargement of airspaces distal to the terminal bronchioles. This leads to a dramatic decline in the alveolar surface area available for gas exchange. Furthermore, loss of alveoli leads to airflow limitation by 2 mechanisms. First, loss of the alveolar walls results in a decrease in elastic recoil, which leads to airflow limitation. Second, loss of the alveolar supporting structure leads to airway narrowing, which further limits airflow.
Emphysema has 3 morphologic patterns:
- Centriacinar
- Panacinar
- Distal acinar, or paraseptal
Centriacinar emphysema is characterized by focal destruction limited to the respiratory bronchioles and the central portions of the acini. This form of emphysema is associated with cigarette smoking and is typically most severe in the upper lobes.
Panacinar emphysema involves the entire alveolus distal to the terminal bronchiole. The panacinar type is typically most severe in the lower lung zones and generally develops in patients with homozygous alpha1-antitrypsin (AAT) deficiency.
Distal acinar emphysema, or paraseptal emphysema, is the least common form and involves distal airway structures, alveolar ducts, and sacs. This form of emphysema is localized to fibrous septa or to the pleura and leads to formation of bullae (as seen in the images below). The apical bullae may cause pneumothorax. Paraseptal emphysema is not associated with airflow obstruction.
 Gross pathology of advanced emphysema. Large bullae are present on the surface of the lung.
Gross pathology of advanced emphysema. Large bullae are present on the surface of the lung. Gross pathology of a patient with emphysema showing bullae on the surface.
Gross pathology of a patient with emphysema showing bullae on the surface.
The gradual destruction of alveolar septae (shown in the image below) and of the pulmonary capillary bed in emphysema leads to a decreased ability to oxygenate blood. The body compensates with lowered cardiac output and hyperventilation. This V/Q mismatch results in relatively limited blood flow through a fairly well oxygenated lung with normal blood gases and pressures in the lung, in contrast to the situation in chronic bronchitis. Because of low cardiac output, the rest of the body suffers from tissue hypoxia and pulmonary cachexia. Eventually, these patients develop muscle wasting and weight loss and are identified as "pink puffers."
 At high magnification, loss of alveolar walls and dilatation of airspaces in emphysema can be seen.
At high magnification, loss of alveolar walls and dilatation of airspaces in emphysema can be seen.Emphysematous destruction and small airway inflammation
Emphysematous destruction and small airway inflammation often are found in combination in individual patients, leading to the spectrum that is known as COPD. When emphysema is moderate or severe, loss of elastic recoil, rather than bronchiolar disease, is the dominant mechanism of airflow limitation. By contrast, when emphysema is mild, bronchiolar abnormalities are most responsible for the majority of the deficit in lung function. Although airflow obstruction in emphysema is often irreversible, bronchoconstriction due to inflammation accounts for some reversibility. Airflow limitation is not the only pathophysiologic mechanism by which symptoms occur.
Dynamic hyperinflation
Lung volumes, particularly dynamic hyperinflation, have also been shown to play a crucial role in the development of dyspnea perceived during exercise. In fact, the improvement in exercise capacity brought about by several treatment modalities, including bronchodilators, oxygen therapy, lung volume reduction surgery (LVRS), and maneuvers learned in pulmonary rehabilitation, is more likely due to delaying dynamic hyperinflation rather than improving the degree of airflow obstruction. Additionally, hyperinflation (defined as the ratio of inspiratory capacity to total lung capacity [IC/TLC]) has been shown to predict survival better than forced expiratory volume in 1 second (FEV1).
Etiology
Cigarette smoking
The primary cause of COPD is exposure to tobacco smoke. Overall, tobacco smoking accounts for as much as 90% of COPD risk.
Cigarette smoking induces macrophages to release neutrophil chemotactic factors and elastases, which lead to tissue destruction. Clinically significant COPD develops in 15% of cigarette smokers, although this number is believed to be an underestimate. Age of initiation of smoking, total pack-years, and current smoking status predict COPD mortality.
People who smoke have an increased annual decline in FEV1: the physiologic normal decline in FEV1 is estimated to be 20-30 ml/y, but the rate of decline in COPD patients is generally 60 ml/y or greater.
Secondhand smoke, or environmental tobacco smoke, increases the risk of respiratory infections, augments asthma symptoms, and causes a measurable reduction in pulmonary function.
A study by Nagelmann et al concluded that lung function deviation and lung structural changes are present in people who smoke cigarettes before the clinical signs of airway obstruction reveal them.[19] These changes can be detected by body plethysmography and diffusing capacity measurement with routine spirometry.
Environmental factors
COPD does occur in individuals who have never smoked. Although the role of air pollution in the etiology of COPD is unclear, the effect is small when compared with that of cigarette smoking. In developing countries, the use of biomass fuels with indoor cooking and heating is likely to be a major contributor to the worldwide prevalence of COPD. Long-term exposure to traffic-related air pollution may be a factor in COPD in patients with diabetes and asthma.
Airway hyperresponsiveness
Airway hyperresponsiveness (ie, Dutch hypothesis) stipulates that patients who have nonspecific airway hyperreactivity and who smoke are at increased risk of developing COPD with an accelerated decline in lung function. Nonspecific airway hyperreactivity is inversely related to FEV1 and may predict a decline in lung function.
The possible role of airway hyperresponsiveness as a risk factor for the development of COPD in people who smoke is unclear. Moreover, bronchial hyperreactivity may result from airway inflammation observed with the development of smoking-related chronic bronchitis. This may contribute to airway remodeling, leading to a more fixed obstruction, as is seen in persons with COPD.
Alpha1-antitrypsin deficiency
Alpha1-antitrypsin (AAT) is a glycoprotein member of the serine protease inhibitor family that is synthesized in the liver and is secreted into the bloodstream. The main purpose of this 394-amino-acid, single-chain protein is to neutralize neutrophil elastase in the lung interstitium and to protect the lung parenchyma from elastolytic breakdown. Severe AAT deficiency predisposes to unopposed elastolysis with the clinical sequela of an early onset of panacinar emphysema. To see complete information on Alpha1-Antitrypsin Deficiency
AAT deficiency is the only known genetic risk factor for developing COPD and accounts for less than 1% of all cases in the United States. Severe AAT deficiency leads to premature emphysema at an average age of 53 years for nonsmokers and 40 years for smokers.
Nearly 24 variants of the AAT molecule have been identified, and all are inherited as codominant alleles. The common M allele (PiM) may be found in 90% of people, and homozygous (PiMM) phenotypes produce serum levels within the reference range. The homozygous PiZZ state is the most common deficiency state and accounts for 95% of people in the severely deficient category.
Intravenous drug use
Emphysema occurs in approximately 2% of persons who use intravenous (IV) drugs. This is attributed to pulmonary vascular damage that results from the insoluble filler (eg, cornstarch, cotton fibers, cellulose, talc) contained in methadone or methylphenidate.
The bullous cysts found in association with IV use of cocaine or heroin occur predominantly in the upper lobes. In contrast, methadone and methylphenidate injections are associated with basilar and panacinar emphysema.
Immunodeficiency syndromes
Human immunodeficiency virus (HIV) infection has been found to be an independent risk factor for COPD, even after controlling for confounding variables such as smoking, IV drug use, race, and age.[22]
Apical and cortical bullous lung damage occurs in patients who have autoimmune deficiency syndrome and Pneumocystis carinii infection. Reversible pneumatoceles are observed in 10-20% of patients with this infection.
Vasculitis syndrome
Hypocomplementemic vasculitis urticaria syndrome (HVUS) may be associated with obstructive lung disease. Other manifestations include angioedema, nondeforming arthritis, sinusitis, conjunctivitis, and pericarditis.
Connective tissue disorders
Cutis laxa is a disorder of elastin that is characterized most prominently by the appearance of premature aging. The disease usually is congenital, with various forms of inheritance (ie, dominant, recessive). Precocious emphysema has been described in association with cutis laxa as early as the neonatal period or infancy. The pathogenesis of this disorder includes a defect in the synthesis of elastin or tropoelastin.
Marfan syndrome is an autosomal dominant inherited disease of type I collagen characterized by abnormal length of the extremities, subluxation of the lenses, and cardiovascular abnormality. Pulmonary abnormalities, including emphysema, have been described in approximately 10% of patients.
Ehlers-Danlos syndrome refers to a group of inherited connective tissue disorders with manifestations that include hyperextensibility of the skin and joints, easy bruisability, and pseudotumors; it has also been associated with a higher prevalence of COPD.
Salla disease
Salla disease is an autosomal recessive storage disorder described in Scandinavia; the disease is characterized by intralysosomal accumulation of sialic acid in various tissues. The most important clinical manifestations are severe mental retardation, ataxia, and nystagmus. Precocious emphysema has been described and likely is secondary to impaired inhibitory activity of serum trypsin.
Epidemiology
The National Health Interview Survey reports the prevalence of emphysema at 18 cases per 1000 persons and chronic bronchitis at 34 cases per 1000 persons. While the rate of emphysema has stayed largely unchanged since 2000, the rate of chronic bronchitis has decreased. Another study estimates a prevalence of 10.1% in the United States. However, the exact prevalence of COPD in the United States is believed to be underestimated. This is largely due to the fact that it is an underdiagnosed (and undertreated) disease, because most patients do not present for medical care until the disease is in a late stage.
The exact prevalence of COPD worldwide is largely unknown, but estimates have varied from 7-19%. The Burden of Obstructive Lung Disease (BOLD) study found a global prevalence of 10.1%. Men were found to have a pooled prevalence of 11.8% and women 8.5%. The numbers vary in different regions of the world. Cape Town, South Africa, has the highest prevalence, affecting 22.2% of men and 16.7% of women.
Hannover, Germany, on the other hand, has the lowest prevalence, of 8.6% for men and 3.7% for women. The differences can be explained in part by site and sex differences in the prevalence of smoking. As noted above, these reports are widely believed to be underestimates because COPD is known to be underdiagnosed and undertreated. Additionally, the prevalence in women is believed to be increasing.
Although current rates of COPD in men are higher than the rates in women, the rates in women have been increasing. COPD occurs predominantly in individuals older than age 40 years.
Severe, early onset disease likely represents a distinct genotype and is more commonly seen in females, African Americans, and those with a maternal family history of COPD.
A study by Mintz et al estimated the prevalence of unidentified COPD. Using the Lung Function Questionnaire (LFQ) and spirometry results, the study determined that approximately 1 in 5 patients (21%) aged 30 years or older with a history of smoking for 10 years or longer seen in a primary care center is likely to have COPD.
In a study by Spitzer et al in Germany, airflow limitation as measured by spirometry was significantly more common in adults with posttraumatic stress disorder than in controls. Results were adjusted for lifestyle, clinical, and sociodemographic factors.
Prognosis
COPD is the third leading cause of death in the United States. In terms of COPD as the underlying cause of death, absolute mortality rates for US patients aged 25 years or older (2005) were 77.3 deaths per 100,000 males and 56.0 deaths per 100,000 females, or 64.3 persons per 100,000 overall. Internationally, overall mortality rates from COPD vary markedly, from more than 400 deaths per 100,000 males aged 65-74 years in Romania to fewer than 100 deaths per 100,000 population in Japan.
The FEV1 was used to predict outcome in COPD until other factors were identified to play a role in determining the outcome of COPD patients. These discoveries resulted in the creation of the multidimensional BODE index (body mass index, obstruction [FEV1], dyspnea [modified Medical Research Council dyspnea scale], and exercise capacity [6MWD]). This index was developed to assess an individual’s risk of death or hospitalization.
Prognosis is based on a point system, with all 4 factors used to determine the score, as follows:
- Body mass index: greater than 21 = 0 points; less than 21 = 1 point
- FEV 1 (postbronchodilator percent predicted): greater than 65% = 0 points; 50-64% = 1 point; 36-49% = 2 points; less than 35% = 3 points
- Modified Medical Research Council (MMRC) dyspnea scale: MMRC 0 = dyspneic on strenuous exercise (0 points); MMRC 1 = dyspneic on walking a slight hill (0 points); MMRC 2 = dyspneic on walking level ground, must stop occasionally due to breathlessness (1 point); MMRC 3 = dyspneic after walking 100 yards or a few minutes (2 points); MMRC 4 = cannot leave house; dyspneic doing activities of daily living (3 points)
- Six-minute walking distance: greater than 350 meters = 0 points; 250-349 meters = 1 point; 150-249 meters = 2 points; less than 149 meters = 3 points
The approximate 4-year survival based on the point system above is as follows:
- 0-2 points = 80%
- 3-4 points = 67%
- 5-6 points = 57%
- 7-10 points = 18%
The use of a clinical scoring system reinforces that determinants of prognosis in COPD remain multifactorial. Waschki et al argued that objective assessments of physical activity, including 6-minute walk test results, are best able to predict mortality. However, additional socioeconomic factors also likely play a role in COPD prognosis; for example, a retrospective cohort study highlighted the increased risk of COPD-related mortality in patients who reside in isolated rural areas.
A study by Sundh et al determined that the Clinical COPD Questionnaire (CCQ), which estimates quality of life in patients with COPD, is effective. The CCQ identified that heart disease, depression, and underweight status are independently associated with lower health-related quality of life in patients with COPD.
In a multicenter, prospective, observational study of 201 consecutive patients with moderate-to-severe COPD, Martinez-Garcia et al reported that in addition to smoking, pulmonary hypertension, and declining lung function, all of which are known risk factors for mortality in patients with COPD, bronchiectasis, which is common in patients with moderate-to-severe COPD, is independently associated with increased risk of all-cause mortality.
In this study, those who had bronchiectasis were found to be 2.5 times more likely to die than those who did not. Bronchiectasis remained an independent factor after adjustment for dyspnea, partial pressure of oxygen, body mass index, presence of potentially pathogenic microorganisms in sputum, presence of daily sputum production, number of severe exacerbations and peripheral albumin, and ultrasensitive C-reactive protein concentrations.
History
Most patients with chronic obstructive pulmonary disease (COPD) seek medical attention late in the course of their disease. Patients often ignore the symptoms because they start gradually and progress over the course of years. Patients often modify their lifestyle to minimize dyspnea and ignore cough and sputum production. With retroactive questioning, a multiyear history can be elicited.
Patients typically present with a combination of signs and symptoms of chronic bronchitis, emphysema, and reactive airway disease. These include cough, worsening dyspnea, progressive exercise intolerance, sputum production, and alteration in mental status. Symptoms include the following:
- Productive cough or acute chest illness
- Breathlessness
- Wheezing
Systemic manifestations (decreased fat-free mass, impaired systemic muscle function, osteoporosis, anemia, depression, pulmonary hypertension, cor pulmonale, left-sided heart failure
A productive cough or an acute chest illness is common. The cough usually is worse in the mornings and produces a small amount of colorless sputum.
Breathlessness is the most significant symptom, but it usually does not occur until the sixth decade of life (although it may occur much earlier). By the time the FEV1has fallen to 50% of predicted, the patient is usually breathless upon minimal exertion. In fact, the FEV1 is the most common variable used to grade the severity of COPD, although it is not the best predictor of mortality.
Wheezing may occur in some patients, particularly during exertion and exacerbations.
The value of patient history and physical examination was addressed in the 2011 update to the American College of Physicians/American College of Chest Physicians/American Thoracic Society/European Respiratory Society (ACP/ACCP/ATS/ERS) guideline for diagnosis and management of stable COPD. According to the 2011 guideline, a history of more than 40 pack-years of smoking was the best single predictor of airflow obstruction; however, the most helpful information was provided by a combination of the following 3 signs :
- Self-reported smoking history of more than 55 pack-years
- Wheezing on auscultation
- Self-reported wheezing
If all 3 signs are absent, airflow obstruction can be nearly ruled out.
With disease progression, intervals between acute exacerbations become shorter, and each exacerbation may be more severe. The rate of COPD exacerbations appears to reflect an independent susceptibility phenotype.
COPD is now known to be a disease with systemic manifestations, and the quantification of these manifestations has proved to be a better predictor of mortality than lung function alone. Many patients with COPD may have decreased fat-free mass, impaired systemic muscle function, osteoporosis, anemia, depression, pulmonary hypertension, cor pulmonale, and even left-sided heart failure. Depression is not uncommon in subjects with COPD.
In addition, COPD appears to increase the risk for mild cognitive impairment (MCI). Investigators from the Mayo Clinic Study of Aging—a population-based, cross-sectional study of 1,927 participants—reported an association between COPD and an increased risk of having MCI, MCI subtypes, and memory loss in elderly patients. They also observed a dose-response relationship between COPD duration and an increased risk for cognitive problems.
The prevalence of MCI was significantly higher in patients with COPD (n = 288) (27%) than in those without COPD (15%), and there was a nearly twofold higher odds ratio (1.87) for MCI in patients with COPD. Moreover, the odds ratio increased from 1.6 in patients with COPD for 5 years or less to 2.1 in those who had COPD for longer than 5 years.
Some important clinical and historical differences may help distinguish between the types of COPD. Classic findings for patients with chronic bronchitis include productive cough with gradual progression to intermittent dyspnea; frequent and recurrent pulmonary infections; and progressive cardiac/respiratory failure with edema and weight gain. Classic findings for patients with emphysema include a long history of progressive dyspnea with late onset of nonproductive cough; occasional mucopurulent relapses; and eventual cachexia and respiratory failure.
Physical Examination
The sensitivity of a physical examination in detecting mild to moderate COPD is relatively poor; however, physical signs are quite specific and sensitive for severe disease. Patients with severe disease experience tachypnea and respiratory distress with simple activities.
The respiratory rate increases in proportion to disease severity. Use of accessory respiratory muscles and paradoxical indrawing of lower intercostal spaces is evident (known as the Hoover sign). In advanced disease, cyanosis, elevated jugular venous pulse (JVP), and peripheral edema can be observed.
Thoracic examination reveals the following:
- Hyperinflation (barrel chest)
- Wheezing – Frequently heard on forced and unforced expiration
- Diffusely decreased breath sounds
- Hyperresonance on percussion
- Prolonged expiration
In addition, coarse crackles beginning with inspiration may be heard.
Certain characteristics allow differentiation between disease that is predominantly chronic bronchitis and that which is predominantly emphysema.
Chronic bronchitis characteristics include the following:
- Patients may be obese
- Frequent cough and expectoration are typical
- Use of accessory muscles of respiration is common
- Coarse rhonchi and wheezing may be heard on auscultation
- Patients may have signs of right heart failure (ie, cor pulmonale), such as edema and cyanosis
Emphysema characteristics include the following:
- Patients may be very thin with a barrel chest
- Patients typically have little or no cough or expectoration
- Breathing may be assisted by pursed lips and use of accessory respiratory muscles; patients may adopt the tripod sitting position
- The chest may be hyperresonant, and wheezing may be heard
- Heart sounds are very distant
- Overall appearance is more like classic COPD exacerbation
Staging
The severity of airflow obstruction was the primary means of staging COPD until the American Thoracic Society (ATS) provided criteria for staging COPD based on the presence of obstruction (ratio of FEV1 to forced vital capacity [FEV1/FVC] < 70%) and its severity as measured by percent of predicted FEV1. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification took staging one step further by incorporating the presence of respiratory failure into its most severe stage.[5] Furthermore, GOLD provided guidelines for therapy based on stage.
ATS and GOLD criteria for assessing the severity of airflow obstruction (based on the percent predicted postbronchodilator FEV1 when the FEV1/FVC is < 70%) are as follows:
- Stage I (mild) - FEV 1 80% or greater of predicted
- Stage II (moderate) - FEV 1 50-79% of predicted
- Stage III (severe) - FEV 1 30-49% of predicted
- Stage IV (very severe) - FEV 1 less than 30% of predicted or FEV 1 less than 50% and chronic respiratory failure
However, these staging systems have limited utility in predicting mortality. The recognition that COPD is a systemic disease has helped in developing criteria that are better at predicting mortality than is assessment of airway obstruction alone. A widely used system for COPD prognosis is the BODE index (body mass index, obstruction [FEV1], dyspnea [modified Medical Research Council dyspnea scale], and exercise capacity [6MWD]).
Dsisease Workup
The defining feature of COPD is irreversible airflow limitation during forced expiration. This may result from a loss of elastic recoil due to lung tissue destruction or from an increase in the resistance of the conducting airways. The formal diagnosis of COPD is made with spirometry; when the ratio of forced expiratory volume in 1 second over forced vital capacity (FEV1/FVC) is less than 70% of that predicted for a matched control, it is diagnostic for a significant obstructive defect. Other studies, including laboratory studies and imaging, are particularly important during acute exacerbations of disease.
The 2011 ICSI guidelines also emphasize the importance of spirometry in diagnosing patients.
No blood-based biomarkers are accepted in COPD. However, a study by Sin et al investigated the use of serum pulmonary and activation-regulated chemokine (PARC/CCL-18) as a potential biomarker. The study determined hat PARC/CCL-18 levels are elevated in COPD and track clinical outcomes.
A large retrospective review from the United Kingdom found that in the 5 years preceding a diagnosis of COPD, primary care practitioners and specialists had missed opportunities to diagnose the disease in 85% of patients. Of the almost 39,000 patients in the study, 32,900 had presented with clinical or test findings consistent with early COPD. Missed opportunities included lower respiratory tract consultations resulting in a prescription for antibiotics or oral steroids and chest radiography not leading to a COPD diagnosis. Women were more likely to be underdiagnosed than men.
Arterial Blood Gas Analysis
Arterial blood gas (ABG) analysis provides the best clues as to acuteness and severity of disease exacerbation.
Patients with mild COPD have mild to moderate hypoxemia without hypercapnia. As the disease progresses, hypoxemia worsens and hypercapnia may develop, with the latter commonly being observed as the FEV1 falls below 1 L/s or 30% of the predicted value. Lung mechanics and gas exchange worsen during acute exacerbations.
In general, renal compensation occurs even in chronic CO2 retainers (ie, bronchitics); thus, pH usually is near normal. Generally, consider any pH below 7.3 to be a sign of acute respiratory compromise.
Serum Chemistries
Patients with COPD tend to retain sodium. In addition, serum potassium should be monitored carefully, because diuretics, beta-adrenergic agonists, and theophylline act to lower potassium levels.
Beta-adrenergic agonists also increase renal excretion of serum calcium andmagnesium, which may be important in the presence of hypokalemia.
Chronic respiratory acidosis leads to compensatory metabolic alkalosis. In the absence of blood gas measurements, bicarbonate levels are useful for following disease progression.
Alpha1-Antitrypsin
Measure alpha1-antitrypsin (AAT) in all patients younger than 40 years or in those with a family history of emphysema at an early age. The diagnosis of severe AAT deficiency is confirmed when the serum level falls below the protective threshold value of 11 mmol/L (ie, in the range of 3-7 mmol/L).
Specific phenotyping is reserved for patients in whom serum levels are 7-11 mmol/L or when genetic counseling or family analysis is needed.
Sputum Evaluation
In persons with stable chronic bronchitis, the sputum is mucoid and macrophages are the predominant cells. With an exacerbation, sputum becomes purulent because of the presence of neutrophils. Although the quality of sputum can vary between patients in chronic stable disease, an increase in the quantity of sputum production is often a sign of an acute exacerbation.
A mixture of organisms often is visible with Gram stain. The pathogens cultured most frequently during exacerbations are Streptococcus pneumoniae and Haemophilus influenzae.Moraxella catarrhalis is also a common organism, and Pseudomonas aeruginosa can be seen in patients with severe obstruction.
B-Type Natriuretic Peptide
Human B-type natriuretic peptide (BNP) binds to particulate guanylate cyclase receptors of vascular smooth muscle and endothelial cells. Binding to the receptors causes an increase in cyclic guanosine monophosphate (GMP), which serves as a secondary messenger to dilate veins and arteries.
By measuring BNP, it was thought that the ability to differentiate between CHF and COPD exacerbations would become much easier. However, clinical observation and research have shown that in cases of mild CHF exacerbation, differentiation between CHF and COPD is still not straightforward. A mild elevation of BNP must be taken in context with the overall clinical picture.
New biomarkers such as pro-BNP peptide assays are in development and may prove helpful in differentiating COPD from CHF exacerbations in the future.
Chest Radiography
As demonstrated in the images below, frontal and lateral chest radiographs of patients with emphysema reveal signs of hyperinflation, including flattening of the diaphragm, increased retrosternal air space, and a long, narrow heart shadow. Rapidly tapering vascular shadows accompanied by hyperlucency of the lungs are other signs of emphysema.
Chronic bronchitis is associated with increased bronchovascular markings and cardiomegaly.
With complicating pulmonary hypertension, the hilar vascular shadows are prominent, with possible right ventricular enlargement and opacity in the lower retrosternal air space.
 Posteroanterior (PA) and lateral chest radiograph in a patient with severe chronic obstructive pulmonary disease (COPD). Hyperinflation, depressed diaphragm, increased retrosternal space, and hypovascularity of lung parenchyma are demonstrated.
Posteroanterior (PA) and lateral chest radiograph in a patient with severe chronic obstructive pulmonary disease (COPD). Hyperinflation, depressed diaphragm, increased retrosternal space, and hypovascularity of lung parenchyma are demonstrated. A lung with emphysema shows increased anteroposterior (AP) diameter, increased retrosternal airspace, and flattened diaphragm on lateral chest radiograph.
A lung with emphysema shows increased anteroposterior (AP) diameter, increased retrosternal airspace, and flattened diaphragm on lateral chest radiograph. A lung with emphysema shows increased anteroposterior (AP) diameter, increased retrosternal airspace, and flattened diaphragm on posteroanterior chest radiograph.
A lung with emphysema shows increased anteroposterior (AP) diameter, increased retrosternal airspace, and flattened diaphragm on posteroanterior chest radiograph.Computed Tomography
High-resolution CT (HRCT) scanning is more sensitive than standard chest radiography and is highly specific for diagnosing emphysema (outlined bullae are not always visible on a radiograph).
HRCT scanning may provide an adjunct means of diagnosing various forms of COPD (ie, lower lobe disease may suggest AAT deficiency) and may help the clinician to determine whether surgical intervention would benefit the patient. (See the CT image below.)
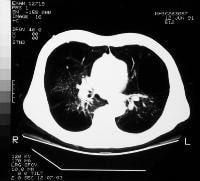 Severe bullous disease as seen on a computed tomography (CT) scan in a patient with chronic obstructive pulmonary disease (COPD).
Severe bullous disease as seen on a computed tomography (CT) scan in a patient with chronic obstructive pulmonary disease (COPD).Two-Dimensional Echocardiography
Many patients with long-standing COPD develop secondary pulmonary hypertension from chronic hypoxemia and vascular remodeling. This may result in eventual right-sided heart failure (cor pulmonale). However, even with severe COPD, the degree of pulmonary hypertension is usually only mild to moderate. Findings of severe pulmonary hypertension on echocardiogram or cardiac catheterization warrant further workup.
Two-dimensional echocardiography may be helpful as a screening tool to estimate pulmonary arterial systolic pressure and right ventricular systolic function, although formal cardiac catheterization is necessary to accurately confirm the diagnosis.
Pulmonary Function Tests
Pulmonary function tests are essential for the diagnosis and assessment of the severity of disease, and they are helpful in following its progress. (See the images below.) FEV1 is a reproducible test and is the most commonly used index of airflow obstruction.
In addition to the spirometry findings that define the disease, lung volume measurements often show an increase in total lung capacity, functional residual capacity, and residual volume. The vital capacity often decreases. Dynamic hyperinflation during exercise is now thought be a greater contributor to the sensation of dyspnea than airflow obstruction alone (as measured by FEV1).
As many as 30% of patients have an increase in FEV1 of 15% or more after inhalation of a bronchodilator. However, the absence of bronchodilator response does not justify withholding therapy.
Carbon monoxide diffusing capacity is decreased in proportion to the severity of emphysema.
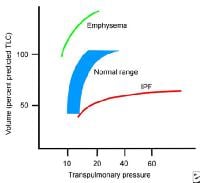 Pressure volume curve comparing lungs with emphysema, lungs with restrictive disease, and normal lungs.
Pressure volume curve comparing lungs with emphysema, lungs with restrictive disease, and normal lungs.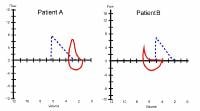 Flow volume curve of a patient with emphysema shows marked decrease in expiratory flow, hyperinflation, and air trapping (patient B) compared with a patient with restrictive lung disease, who has reduced lung volumes and preserved flow (patient A).
Flow volume curve of a patient with emphysema shows marked decrease in expiratory flow, hyperinflation, and air trapping (patient B) compared with a patient with restrictive lung disease, who has reduced lung volumes and preserved flow (patient A).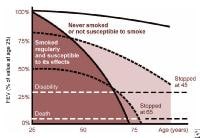 Forced expiratory volume in 1 second (FEV1) can be used to evaluate the prognosis in patients with emphysema. The benefit of smoking cessation is shown here because the deterioration in lung function parallels that of a nonsmoker, even in late stages of the disease. Redrawn from Fletcher C, Peato R. The natural history of chronic airflow obstruction. Br Med J 1977; 1: 1645-1648.
Forced expiratory volume in 1 second (FEV1) can be used to evaluate the prognosis in patients with emphysema. The benefit of smoking cessation is shown here because the deterioration in lung function parallels that of a nonsmoker, even in late stages of the disease. Redrawn from Fletcher C, Peato R. The natural history of chronic airflow obstruction. Br Med J 1977; 1: 1645-1648.
Using lung function thresholds of 80% predicted and fixed cut points to determine whether a test result is abnormal could result in the misdiagnosis of more than 20% of patients referred for pulmonary function testing. This misclassification can be avoided by using the lower limit of normal--;based 95% confidence interval.
Six-Minute Walking Distance
The distance walked in 6 minutes (6MWD) is a good predictor of all-cause and respiratory mortality in patients with moderate COPD. Patients with COPD who desaturate during the 6MWD have a higher mortality rate than do those who do not desaturate.
Consequently, this test is used as a part of the BODE index (body mass index, obstruction [FEV1], dyspnea [modified Medical Research Council dyspnea scale], and exercise capacity [6MWD]), which was designed to help predict mortality in COPD patients.
Other Studies
Pulse oximetry does not offer as much information as arterial blood gas (ABG)analysis. However, when combined with clinical observation, this test can be a powerful tool for instant feedback on a patient's status.
Electrocardiography
Coexisting cardiac disease is highly likely in patients with COPD. Electrocardiography can be used in establishing that hypoxia is not resulting in cardiac ischemia and that the underlying cause of respiratory difficulty is not cardiac in nature.
Right-Sided Heart catheterization
If pulmonary hypertension is suspected based on clinical findings or on estimates from 2-dimensional echocardiography, then right-sided heart catheterization may be performed to measure pulmonary artery pressures directly and to gauge the response to vasodilators.
Hematocrit
Chronic hypoxemia may lead polycythemia. A hematocrit greater than 52% in men or 47% in women is indicative of polycythemia. Patients should be evaluated for hypoxemia at rest, with exertion, or during sleep. Correction of hypoxemia should reduce secondary polycythemia in patients who have quit smoking.
Treatment and Management
The goal of COPD management is to improve a patient’s functional status and quality of life by preserving optimal lung function, improving symptoms, and preventing the recurrence of exacerbations. Currently, no treatments aside from lung transplantation have been shown to significantly improve lung function or decrease mortality. Once the diagnosis of COPD is established, it is important to educate the patient about the disease and to encourage his or her active participation in therapy.
Results of a randomized controlled trial showed that a comprehensive disease management strategy, which included a patient education session, a self-treatment plan for exacerbations, and a monthly follow-up call from a case manager, is associated with a lower hospitalization rate and fewer emergency department visits. A study by Dewan et al determined that a multicomponent disease management program in patients with COPD was cost-effective, saving $593 per patient.
Indications for intensive care admission are confusion, lethargy, respiratory muscle fatigue, worsening hypoxemia, and respiratory acidosis (pH < 7.30), as well as clinical concern for impending or active respiratory failure. (BiPAP can be done on the floor in some hospitals, including widely in the United Kingdom).
Approaches to management include recommendations such as those provided by GOLD:
- Stage I (mild obstruction): Reduction of risk factors (influenza vaccine); short-acting bronchodilator as needed
- Stage II (moderate obstruction): Reduction of risk factors (influenza vaccine); short-acting bronchodilator as needed; long-acting bronchodilator(s); cardiopulmonary rehabilitation
- Stage III (severe obstruction): Reduction of risk factors (influenza vaccine); short-acting bronchodilator as needed; long-acting bronchodilator(s); cardiopulmonary rehabilitation; inhaled glucocorticoids if repeated exacerbations
- Stage IV (very severe obstruction or moderate obstruction with evidence of chronic respiratory failure): Reduction of risk factors (influenza vaccine); short-acting bronchodilator as needed; long-acting bronchodilator(s); cardiopulmonary rehabilitation; inhaled glucocorticoids if repeated exacerbation; long-term oxygen therapy (if criteria met); consider surgical options such as LVRS and lung transplantation
Oral and inhaled medications are used for patients with stable disease to reduce dyspnea and improve exercise tolerance. Most of the medications used are directed at the following 4 potentially reversible causes of airflow limitation in a disease state that has largely fixed obstruction:
- Bronchial smooth muscle contraction
- Bronchial mucosal congestion and edema
- Airway inflammation
- Increased airway secretions
Diet
Inadequate nutritional status associated with low body weight in patients with COPD is associated with impaired pulmonary status, reduced diaphragmatic mass, lower exercise capacity, and higher mortality rates. Nutritional support is an important part of comprehensive care in patients with COPD.
Bronchodilation
Bronchodilators are the backbone of any COPD treatment regimen. They work by dilating airways, thereby decreasing airflow resistance. This increases airflow and decreases dynamic hyperinflation. Lack of response in pulmonary function testing should not preclude their use. These drugs provide symptomatic relief but do not alter disease progression or decrease mortality.
Beta2 agonists and anticholinergics
The initial choice of agent remains in debate. Historically, beta2 agonists were considered first line and anticholinergics were added as adjuncts. Not surprisingly, studies have shown combination therapy results in greater bronchodilator response and provides greater relief. Monotherapy with either agent and combination therapy with both are acceptable options. The adverse effect profile may help guide therapy. Generally, long-acting bronchodilators are more beneficial than short-acting ones.
Beta2-agonist bronchodilators activate specific B2-adrenergic receptors on the surface of smooth muscle cells, which increases intracellular cyclic adenosine monophosphate (cAMP) and smooth muscle relaxation. Even patients who have no measurable increase in post-bronchodilator expiratory airflow may benefit from treatment with beta2 agonists. The inhaled route is preferred because it minimizes adverse systemic effects. The adverse effects are predictable and include tachycardia and tremors. Although rare, beta2 agonists may also precipitate a cardiac arrhythmia.
Anticholinergic drugs compete with acetylcholine for postganglionic muscarinic receptors, thereby inhibiting cholinergically mediated bronchomotor tone, resulting in bronchodilation. They block vagally mediated reflex arcs that cause bronchoconstriction. Clinical benefit is gained through a decrease in exercise-induced dynamic hyperinflation. These agents are poorly absorbed systemically and are relatively safe. Reported adverse effects include dry mouth, dry eyes, metallic taste, and prostatic symptoms.
In a study of men with COPD aged 66 years or older from Ontario, Canada, acute urinary retention (AUR) was found to be significantly more prevalent in users of inhaled anticholinergic medications (IACs) than in nonusers. The risk of AUR was higher in patients receiving both short-acting and long-acting IACs than in patients using a single IAC, and evidence of benign prostatic hyperplasia also increased the AUR risk.
Inhaled delivery of medications is preferred over the oral route to help minimize potential adverse effects. Some patients may have difficulty achieving effective delivery of the medication using a metered-dose inhaler; use of a spacer or nebulizer may be beneficial in these patients.
The use of newly prescribed inhaled long-acting beta-agonist and long-acting anticholinergic drugs for COPD was associated with a 31% increased risk of experiencing a cardiovascular event in a recent nested case-control analysis of a retrospective cohort study. Both agents showed an increased risk of acute coronary syndrome and heart failure, but not arrhythmias or stroke. With both agents, the risk of events was highest within the first 2 or 3 weeks of initiating treatment. There was no significant difference in events between the 2 treatments.
In 2013, the results from the SPARK trial showed that in patients with severe COPD, a once-daily fixed-dose combination of indacaterol (a beta2 agonist) and glycopyrronium (a muscarinic antagonist) can improve lung functioning and reduce exacerbations, as compared with monotherapy with either glycopyrronium or tiotropium (both of which are muscarinic antagonists).
Also in 2013, indacaterol and tiotropium were shown to be equally effective in a 52-week, randomized, blinded, parallel-group study consisting of more than 3400 patients with severe COPD who had had at least one exacerbation in the past year. Results from use of the 2 agents demonstrated similar improvements in baseline dyspnea and health status, with similar safety profiles.
Patients treated with indacaterol had a 29% higher exacerbation rate, but needed rescue medication less frequently than patients treated with tiotropium. In both groups, improvements were observed from baseline in trough FEV1 at week 12 (0.114 L with indacaterol and 0.126 L with tiotropium) and at week 52 (0.073 L with indacaterol and 0.092 L with tiotropium).
Umeclidinium bromide and vilanterol (Anoro Ellipta) is a long-acting muscarinic antagonist (LAMA) and long-acting beta2-agonist (LABA) inhalation powder approved by the FDA for long-term maintenance of COPD. . Approval was based on a series of dose-ranging studies in more than 2400 patients—two 6-month, placebo-controlled efficacy and safety studies; two 6-month, active-controlled efficacy and safety studies; and a 12-month safety study.
This agent carries a boxed warning regarding use of LABAs and an increased risk of asthma-related death. Umeclidinium and vilanterol inhalation powder is not approved for asthma therapy, and it is not meant to be used as rescue therapy for sudden breathing problems (eg, acute bronchospasm). Serious adverse effects include paradoxical bronchospasm, cardiovascular effects, acute narrow-angle glaucoma, and worsening of urinary retention.
Olodaterol inhaled (Stirverdi Respimat) was approved by the FDA in July, 2014, for maintenance bronchodilator treatment in patients with COPD. Olodaterol is a long-acting beta2 agonist (LABA) that activates specific β2-adrenergic receptors on the surface of smooth muscle cells, which increases intracellular cAMP and smooth muscle relaxation. Approval was based on data from more than 3,000 patients with COPD studied over a 48-week period. Results demonstrated the long-term efficacy (eg, improved FEV1 at 0-3 hr and trough FEV1) and safety of once-daily olodaterol 5 mcg in patients with moderate to very severe COPD continuing with usual-care maintenance therapy.
Tiotropium
Although the results of the Understanding Potential Long Term Impacts on Function With Tiotropium (UPLIFT) trial did not show a change in the rate of decline of FEV1 or mortality when compared with placebo, it did show a significant reduction in the frequency of COPD exacerbations and hospitalizations and an improvement in quality of life.
Evidence is mounting of the efficacy of tiotropium over long-acting beta agonists. Two large, randomized trials have compared tiotropium, salmeterol (Serevent), and placebo. Both studies showed greater improvement in lung function, dyspnea, and quality of life in the tiotropium group versus the salmeterol group. A study by Brusasco et al also showed a delay in first exacerbations and fewer exacerbations per year in the tiotropium group.
A 1-year, randomized, double-blind, double-dummy, parallel group study by Vogelmeier et al determined that tiotropium is more effective than salmeterol in preventing exacerbations in patients with moderate-to-very-severe COPD.
Tiotropium is available in a capsule dosage form containing a dry powder for oral inhalation via the HandiHaler inhalation device. For adults, the contents of 1 capsule (18 mcg) are inhaled every day via the HandiHaler device. Contraindications, drug interactions, and adverse effects are similar to those of ipratropium.
A systematic review and meta-analysis by Singh et al of 5 randomized controlled trials of the Respimat tiotropium mist inhaler in patients with COPD found a 52% increased risk of mortality (all cause) versus placebo. A randomized study comparing the Respimat mist inhaler to the HandiHaler inhalation device is ongoing as of August 2011.
Aclidinium
Aclidinium (Tudorza Pressair), a long-acting, antimuscarinic (M3) metered-dose inhaler was approved by the FDA in July 2012. Approval was based on randomized, placebo-controlled, clinical trials involving 1276 patients aged >40 years with COPD. The mean 12-week predose FEV1 improvements vs placebo were 0.12 L, 0.07 L, and 0.11 L (P< 0.001) in the trials, with a 24-week improvement of 0.13 L in the 6-month trial. Mean peak improvements in lung function (FEV1) assessed after the first dose were similar to those observed at week 12 in each study.
Umeclidinium bromide
Umeclidinium bromide blocks the action of acetylcholine at muscarinic receptors in the bronchial airways (M3) by preventing increase in intracellular calcium concentration, leading to relaxation of airway smooth muscle. It is available in the United States as a combination inhaled powder with vilanterol (Anoro Ellipta), and is the first once-daily dual bronchodilator approved. It is also available as a single entity inhaler (Incruse Ellipta). Approval for the combination was based on 7 phase III trials including nearly 6,000 patients with COPD. Four 24-week primary efficacy studies (measuring improvement of trough FEV1) and a 52-week long-term safety study were the key studies. Two 12-week exercise/lung function studies provided supportive lung function data and contributed to safety data.
Phosphodiesterase inhibitors
Phosphodiesterase inhibitors increase intracellular cyclic adenosine monophosphate (cAMP) and result in bronchodilation. Additionally, they may improve diaphragm muscle contractility and stimulate the respiratory center.
Theophylline is a nonspecific phosphodiesterase inhibitor and is now limited to use as an adjunctive agent. Theophylline has a narrow therapeutic window with significant adverse effects, including anxiety, tremors, insomnia, nausea, cardiac arrhythmia (particularly multifocal atrial tachycardia), and seizures. It is reserved for patients with hard-to-control COPD or for individuals who are not able to use inhaled agents effectively.
Theophylline is metabolized primarily via the hepatic cytochrome P450 system, a process affected by age, cardiac status, and liver abnormalities. Serum levels of theophylline need to be monitored because of the potential for toxicity. The previously recommended target range of 15-20 mg/dL has now been reduced to 8-13 mg/dL.
Roflumilast (Daliresp) and cilomilast (Ariflo) are second-generation, selective phosphodiesterase-4 inhibitors. They cause a reduction of the inflammatory process (macrophages and CD8+ lymphocytes) in patients with COPD. Cilomilast is completely absorbed following oral administration and has a half-life of approximately 6.5 hours. A dose of 15 mg twice daily has been found to be clinically effective. Nausea, presumably of central origin, is the principal adverse reaction. The FDA advisory panel rejected approval of cilomilast in 2002.
Roflumilast was approved by the FDA in 2011 as a treatment to reduce the risk of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations. In 2 randomized, double-blind, placebo-controlled, multicenter trials, increased FEV1 levels were found in patients who received roflumilast, and the rate of COPD exacerbations was reduced by 17% in these patients.
Endogenous opioids
A study by Gifford et al found that the administration of endogenous opioids modulated the intensity and unpleasantness of breathlessness in patients with COPD.
Beta-adrenergic antagonists (beta-blockers)
Cardiovascular disease is common in patients with COPD and is a leading cause of mortality; however, use of beta-blockers has been discouraged in these patients due to a perceived risk of bronchospasm and concern about inhibition of beta-agonist medication. However, a study by Short et al of 5977 patients in Scotland found that the addition of a cardioselective beta-blocker to established inhaled treatment did not appear to harm pulmonary function and did reduce COPD exacerbations, hospital admissions, and all cause mortality versus controls over a mean follow-up of 4.35 years.
Smoking Cessation
Smoking cessation continues to be the most important therapeutic intervention for COPD. Most patients with COPD have a history of smoking or are currently smoking tobacco products. A smoking cessation plan is an essential part of a comprehensive management plan.
However, the success rates for cessation programs are low because of the addictive power of nicotine. These rates can also be negatively impacted by such factors as conditioned responses to smoking-associated stimuli, poor education, forceful promotional campaigns by the tobacco industry, and psychological problems, including depression. The process of smoking cessation typically requires multiple interventional approaches, including both pharmacologic and non-pharmacologic modalities, and will likely require multiple attempts to maintain success.
The transition from smoking to not smoking occurs in the following 5 stages:
- Precontemplation
- Contemplation
- Preparation
- Action
- Maintenance
Smoking intervention programs include self-help, group, health care provider delivered, workplace, and community programs.
Setting a quit date may be helpful. Physicians and other health care providers should participate in setting the target date and follow-up with respect to maintenance.
Successful cessation programs usually use the following resources and tools:
- Patient education
- A target date to quit
- Follow-up support
- Relapse prevention
- Advice for healthy lifestyle changes
- Social support systems
- Adjuncts to treatment (ie, pharmacologic agents)
Mottillo et al reported meta-analysis results indicating that intensive behavioral interventions, including (but not limited to) individual counseling and telephone counseling, offer considerable benefit for increasing smoking abstinence.
According to the US Preventive Services Task Force (USPSTF) guidelines on preventing tobacco use and tobacco-caused disease, clinicians should ask all adult patients about their use of tobacco products and provide cessation interventions to current users. The guideline engages a "5-A" approach to counseling that includes the following:
- Ask about tobacco use
- Advise to quit through personalized messages
- Assess willingness to quit
- Assist with quitting
- Arrange follow-up care and support
Brief behavioral counseling (< 10 min) and pharmacotherapy are each effective alone—although they are most effective when used together. The USPSTF also advises clinicians to ask all pregnant women, regardless of age, about tobacco use. Those who currently smoke should receive pregnancy-tailored counseling supplemented with self-help materials.
Supervised use of pharmacologic agents is an important adjunct to self-help and group smoking cessation programs.
Nicotine is the ingredient in cigarettes primarily responsible for tobacco addiction. Withdrawal from nicotine may cause unpleasant adverse effects, including anxiety, irritability, difficulty concentrating, anger, fatigue, drowsiness, depression, and sleep disruption. These effects usually occur during the first several weeks.
Nicotine replacement therapies after smoking cessation reduce withdrawal symptoms. If a smoker requires his or her first cigarette within 30 minutes of waking, the individual most likely is highly addicted and would benefit from nicotine replacement therapy.
Several nicotine replacement therapies are available.
Nicotine polacrilex (Nicorette, Nicorette Plus) is a chewing gum and has better quit rates than does counseling alone. Nicotine replacement therapy chewing pieces are marketed in 2 strengths (2 mg, 4 mg). An individual who smokes 1 pack per day should use 4-mg pieces. The 2-mg pieces are to be used by individuals who smoke less than 1 pack per day. Instruct patients to chew hourly and also to chew when needed for their initial cravings for 2 weeks. Gradually reduce the amount chewed over the next 3 months.
Transdermal nicotine patches are readily available for replacement therapy. Long-term success rates are 22-42%, compared with 2-25% for placebo. These agents are well tolerated, and the adverse effects are limited to local skin reactions. Nicotine replacement therapy patches are sold under the trade names NicoDerm, Nicotrol, and Habitrol. Each of these products is dosed with a scheduled graduated decrease in nicotine over 6-10 weeks.
The use of the antidepressant bupropion (Zyban) is also effective for smoking cessation. This nonnicotine aid to smoking cessation enhances central nervous system nonadrenergic function. One study demonstrated that 23% of patients sustained cessation at 1 year, compared with 12% who sustained cessation with the placebo. Bupropion may also be effective in patients who have not been able to quit smoking with nicotine replacement therapy.
Another drug used in smoking cessation is varenicline (Chantix). Varenicline is a partial agonist selective for alpha4, beta2 nicotinic acetylcholine receptors. Its action is thought to result from activity at a nicotinic receptor subtype, where its binding produces agonist activity while simultaneously preventing nicotine binding. Agonistic activity is significantly lower than nicotine.
Management of Inflammation
Inflammation plays a significant role in the pathogenesis of COPD. Systemic and inhaled corticosteroids attempt to temper this inflammation and positively alter the course of disease.
The use of systemic steroids in the treatment of acute exacerbations is widely accepted and recommended, given their high efficacy. A meta-analysis concluded that oral and parenteral corticosteroids significantly reduced treatment failure and the need for additional medical treatment and that they increased the rate of improvement in lung function and dyspnea over the first 72 hours. Note that systemic steroids are not as effective in treating COPD exacerbations as they are in treating bronchial asthma exacerbations.
On the other hand, the use of oral steroids in persons with chronic stable COPD is widely discouraged, given their adverse effects, which include hypertension, glucose intolerance, osteoporosis, fractures, and cataracts. A Cochrane review showed no benefit at low-dose therapy and short-lived benefit with higher doses (>30 mg of prednisolone).
Inhaled corticosteroids provide a more direct route of administration to the airways and, similar to other inhaled agents, are only minimally absorbed. Consequently, aside from the development of thrush, the systemic adverse effects of these medications at standard doses are negligible. Despite the theoretical benefit, the current consensus is that inhaled corticosteroids do not decrease the decline in FEV1, although they have been shown to decrease the frequency of exacerbations and improve quality of life for symptomatic patients with an FEV1 of less than 50%. The 2011 ICSI guidelines conclude that inhaled steroids are appropriate in patients with recurrent exacerbations of COPD.
Inhaled corticosteroids are not recommended as monotherapy and should be added to a regimen that already includes a long-acting bronchodilator. The Towards a Revolution in COPD Health (TORCH) trial showed that a combination of an inhaled corticosteroid and a long-acting beta agonist was more beneficial than inhaled corticosteroids alone. These data suggest that in patients with COPD, inhaled corticosteroids should be used only in conjunction with a long-acting beta agonist.
However, patients treated with inhaled corticosteroids were noted to have an increased rate of pneumonia. The debate continues on the use of inhaled corticosteroids and the risk for pneumonia in patients with COPD. For example, no significant difference in pneumonia risk was found between patients who used inhaled budesonide and those who did not in a study by Sin et al. The authors analyzed data from 7 large clinical trials (n = 7042) of patients with stable COPD who used inhaled budesonide (n = 3801), with or without formoterol (Symbicort or Pulmicort, respectively) or a control regimen (placebo or formoterol alone [Oxis]). Increasing age and decreasing percent of predicted FEV1 were the only variables that were significantly associated with occurrence of pneumonia.
Despite the possible increased risk of pneumonia associated with inhaled corticosteroids, a retrospective cohort study showed that in patients with COPD hospitalized with pneumonia, prior use of inhaled corticosteroids was actually associated with decreased mortality and less mechanical ventilation. Therefore the benefit of inhaled corticosteroids in selected patients will likely continue to outweigh the risks.
Intravenous steroids are often used in high doses for acute exacerbations in the inpatient setting; recent research suggests that there is likely no benefit of IV over oral steroid formulations in acute exacerbations, and thus IV steroids should be reserved only for those patients unable to tolerate oral intake.
Nonsteroidal anti-inflammatory medications have not been shown conclusively to have any benefit in COPD. No response has been shown to medications targeting interleukin-8 and tumor necrosis factor-alpha. Leukotriene inhibitors commonly used in asthma have also not proven to be beneficial in COPD.
However, macrolide antibiotics have been shown to have anti-inflammatory effects in the airways of COPD patients. More specifically, azithromycin has been shown to improve the phagocytic function of pulmonary macrophages and to be a potent anti-inflammatory.
Azithromycin is used clinically for its anti-inflammatory effects in patients with cystic fibrosis and in lung transplantation patients with chronic rejection. Furthermore, one study showed that erythromycin reduced the frequency of exacerbations in 109 patients with COPD treated over 12 months. A subsequent larger randomized controlled trial of 1142 patients showed a slight decrease in COPD exacerbations for patients given azithromycin over 1 year compared with placebo. However, this study also noted an increase in hearing decrements in the patients receiving azithromycin (25% in the treatment group compared with 20% in the placebo group; P =0.04). The noted side effect combined with the concern for breeding antimicrobial resistance continues to prevent widespread use of azithromycin for prevention of COPD exacerbations.
Management of Infection
In patients with COPD, chronic infection or colonization of the lower airways is common from S pneumoniae, H influenzae, and M catarrhalis. In patients with chronic severe airway obstruction, P aeruginosa infection may also be prevalent. The use of antibiotics for the treatment of acute exacerbations is well supported.Patients who benefited most from antibiotic therapy were those with exacerbations that were characterized by at least 2 of the following: increases in dyspnea, sputum production, and sputum purulence (The Winnipeg criteria). No evidence supports the continuous or prophylactic use of antibiotics to prevent exacerbations.
Empiric antimicrobial therapy is recommended in patients with an acute exacerbation (as evidenced by an increase in baseline dyspnea and/or a change in the quantity or quality of cough) and evidence of an infectious process, such as fever, leukocytosis, or an infiltrate on chest radiograph. The antibiotic choice must be comprehensive and should cover all likely pathogens in the context of the clinical setting and local resistance patterns.
In a study by Daniels et al, the addition to doxycycline to corticosteroids was found to somewhat improve treatment for acute exacerbation of COPD (AECOPD). The investigators conducted a randomized, placebo-controlled trial that compared the addition of doxycycline to corticosteroids on clinical outcome in patients hospitalized with AECOPD. In addition to clinical outcome, other parameters were measured, including microbiological outcome, lung function, and systemic inflammation. The 223 patients enrolled in the study represented 265 COPD exacerbations. In addition to systemic corticosteroids, patients received either doxycycline at 200 mg or placebo for 7 days.
Results at 30 days were similar between the 2 groups. At 10 days, the doxycycline group showed superiority in clinical success compared with placebo in the intention-to-treat arm but not in the per-protocol arm. Also at day 10, doxycycline was superior for clinical cure, microbiological outcome, use of open label antibiotics, and symptoms.[81]
Management of Sputum Viscosity and Secretion Clearance
Mucolytic agents reduce sputum viscosity and improve secretion clearance. Viscous lung secretions in patients with COPD consist of mucus-derived glycoproteins and leukocyte-derived DNA.
The oral agent N -acetylcysteine has antioxidant and mucokinetic properties and is used to treat patients with COPD. However, the efficacy of mucolytic agents in the treatment of COPD remains controversial. Although they have been shown to decrease cough and chest discomfort, they have not been shown to improve dyspnea or lung function, and they have also been shown to elicit bronchospasm. When used as an inhalational therapy, N -acetylcysteine should be administered along with a bronchodilator such as albuterol in order to counteract potential induction of bronchospasm.
PPIs for Exacerbations and the Common Cold
In patients with COPD, the addition of a proton pump inhibitor (PPI) to conventional therapy may significantly decrease COPD exacerbations but not the incidence of the common cold, according to a study by Sasaki et al. The investigators conducted a randomized, observer-blind, controlled trial to determine whether PPIs reduce the incidence of common colds in patients with COPD. Patients (n = 100) were assigned to conventional therapy (control group) or conventional therapy plus PPI (lansoprazole [Prevacid] 15 mg/d).
In the study by Sasaki et al, the frequency of common colds and COPD exacerbations was measured, and it was determined that the number of exacerbations per person over 12 months was significantly lower in the PPI group than in the control group. However, no significant difference in the frequency of common colds was observed between the 2 groups. The authors concluded that although the patients who took lansoprazole showed a significant decrease in COPD exacerbations, more definitive clinical trials are required.
Oxygen Therapy and Hypoxemia
COPD is commonly associated with progressive hypoxemia. Oxygen administration reduces mortality rates in patients with advanced COPD because of the favorable effects on pulmonary hemodynamics.
Long-term oxygen therapy improves survival 2-fold or more in hypoxemic patients with COPD, according to 2 landmark trials, the British Medical Research Council (MRC) study and the US National Heart, Lung and Blood Institute’s Nocturnal Oxygen Therapy Trial (NOTT). Hypoxemia is defined as PaO2 (partial pressure of oxygen in arterial blood) of less than 55 mm Hg or oxygen saturation of less than 90%. Oxygen was used for 15-19 hours per day.
Therefore, specialists recommend long-term oxygen therapy for patients with a PaO2 of less than 55 mm Hg, a PaO2 of less than 59 mm Hg with evidence of polycythemia, or cor pulmonale. Reevaluate these patients 1-3 months after initiating therapy, because some patients may not require long-term oxygen.
Many patients with COPD who are not hypoxemic at rest worsen during exertion. Home supplemental oxygen commonly is prescribed for these patients. Oxygen supplementation during exercise can prevent increases in pulmonary artery pressure, reduce dyspnea, and improve exercise tolerance.
In a 2008 study, however, patients with COPD-related hypoxemia and exertional desaturation who completed a program of pulmonary rehabilitation failed to show any benefit in domestic activity, health-related quality of life, or time spent outside of the home when compared with those who received placebo. Hence, the benefits of home ambulatory oxygen for this subset of patients remain controversial.
Oxygen therapy generally is safe. Oxygen toxicity from high inspired concentrations (>60%) is well recognized. Little is known about the long-term effects of low-flow oxygen. However, the increased survival and quality-of-life benefits of long-term oxygen therapy outweigh the possible risks of oxygen toxicity.
Carbon dioxide retention from depression of hypoxic drive has been overemphasized. Despite the widely held belief that too much oxygen causes significant respiratory depression, multiple studies in the literature dispute this view. With administration of oxygen, PaCO2 rises, but not in proportion to the very minor changes in respiratory drive. Carbon dioxide retention is more likely a consequence of ventilation-perfusion mismatching rather than respiratory center depression. While this complication is not common, it is best avoided by titrating oxygen delivery to maintain the PaO2 at 60-65 mm Hg.
The major physical hazards of oxygen therapy are fires or explosions. Patients, family, and other caregivers must be warned not to smoke. Overall, major accidents are rare and can be avoided by good patient and family training.
The continuous-flow nasal cannula is the standard means of oxygen delivery for the stable hypoxemic patient. It is simple, reliable, and generally well tolerated. Each liter of oxygen flow adds 3-4% to the fraction of inspired oxygen (FiO2). Nasal oxygen delivery also is beneficial for most mouth-breathing patients. Humidification generally is not necessary when the patient receives oxygen by nasal cannula at flows of less than 5 L/min. (See the images below.)
 Oxygen therapy via nasal cannula.
Oxygen therapy via nasal cannula. Home supplemental oxygen.
Home supplemental oxygen.
Oxygen-conserving devices function by delivering all of the supplemental oxygen during early inhalation. These devices improve the portability of oxygen therapy and may reduce overall costs. Three distinct oxygen-conserving devices are available: reservoir cannulas, demand-pulse delivery devices, and transtracheal oxygen delivery. Transtracheal oxygen delivery involves the insertion of a catheter percutaneously between the second and third tracheal interspace. Transtracheal oxygen delivery is invasive and requires special training for the physician, the patient, and the caregiver. The procedure has risks as well as medical benefits but has limited application.
NIPPV for hypercapneic respiratory failure
Noninvasive positive-pressure ventilation (NIPPV), as the name suggests, allows the delivery of positive-pressure ventilation without the use of an endotracheal tube. In place of the tube is a tight-fitting nasal or facial mask that is attached to a continuous positive airway pressure (CPAP) or a bilevel positive airway pressure (BiPAP) machine (as seen below). The positive pressure is beneficial in hypercapneic respiratory failure by decreasing the work of breathing, allowing a larger tidal volume for a given respiratory effort, and hence improving alveolar ventilation.
 Bilevel positive airway pressure (BiPAP).
Bilevel positive airway pressure (BiPAP).
NIPPV has been shown to provide significant benefits in selected patients with acute hypercapneic respiratory failure due to COPD, including a reduction in the need for endotracheal intubation, reduced hospital stay, and a mortality benefit. This modality should not be used in patients who are unable to protect their airway, are hemodynamically unstable, have significant secretions, are uncooperative, or have an Acute Physiology and Chronic Health Evaluation (APACHE) score of greater than 29.
Another study suggests that in patients with chronic hypercapneic respiratory failure who are undergoing pulmonary rehabilitation, nocturnal NIPPV may improve quality of life, daytime PaCO2, and exercise tolerance.
In 2011, the Canadian Critical Care Trials Group and the Canadian Critical Care Society Noninvasive Ventilation Guidelines Group issued guidelines encouraging the use of noninvasive ventilation (NIPPV or CPAP) to avoid intubation for patients in acute care with respiratory failure. Key recommendations relevant to COPD include the following:
- NIPPV should be the first-line choice for supporting patients with a severe exacerbation of COPD.
- In facilities with extensive NIPPV experience, patients with COPD can be considered for a trial of early extubation to NIPPV.
- Patients with hypoxemia or acute respiratory distress after undergoing surgery or in immunosuppression can be considered for a trial of NIPPV.
- Routine use of helium-oxygen is not recommended with NIPPV in patients with severe exacerbation of COPD.
Commentary accompanying the Canadian Critical Care guideline urges close patient monitoring and 24-hour availability of an experienced rescue team in case noninvasive ventilation fails and rapid intervention is required.
Vaccination to Reduce Infections
Infections can lead to COPD exacerbations. Vaccinations are a safe and effective modality to reduce infections in susceptible COPD patients. The pneumococcal vaccine should be offered to all patients older than 65 years or to patients of any age who have an FEV1 of less than 40% of predicted. The influenza vaccine should be given annually to all COPD patients.
Alpha1-Antitrypsin Deficiency Treatment
The treatment strategies for AAT deficiency involve reducing the neutrophil elastase burden, primarily by smoking cessation, and augmenting the levels of AAT. Available augmentation strategies include pharmacologic attempts to increase endogenous production of AAT by the liver (ie, danazol, tamoxifen) and administration of purified AAT by periodic intravenous infusion or by inhalation. Tamoxifen can increase endogenous production of AAT to a limited extent, so this may be beneficial in persons with the PISZ phenotype.
Intravenous AAT augmentation therapy is the only available approach that can increase serum levels to greater than 11 mmol/L, the protective threshold. Studies show that the infusions can maintain levels of more than 11 mmol/L, and replacement is administered weekly (60 mg/kg), biweekly (120 mg/kg), or monthly (250 mg/kg).
Purified AAT is currently available in 3 formulations, with trade names of Prolastin, Zemaira, and Aralast, all of which are derived from donor blood. Synthetic formulations of AAT are under development but not yet available. The ability of intravenous AAT augmentation to alter the clinical course of patients with AAT deficiency has not been demonstrated. Uncontrolled observations of patients suggest that the FEV1 may fall at a slower rate in patients who receive AAT replacement.
Inpatient Care
Treatment for acute exacerbation of COPD
Acute exacerbation (AE) COPDs are a major reason for hospital admission in the United States, although mild episodes may be treated in an outpatient setting. Indications for admission include failure of outpatient treatment, marked increase in dyspnea, altered mental status, increase in hypoxemia or hypercapnia, and inability to tolerate oral medications such as antibiotics or steroids. Care must be taken to evaluate for other conditions that may mimic AECOPD.
Patients with COPD are susceptible to many insults that can lead rapidly to an acute deterioration superimposed on chronic disease. AECOPD—an important, but occasionally overlooked, parameter—is defined as worsening of cough, increase in sputum production, change in sputum quality, and increase in dyspnea.
AECOPDs are very common, affecting about 20% of patients with moderate to severe COPD (1.3 events per year in patients with 40-45% of predicted FEV1). Quick and accurate recognition of these patients, along with aggressive and prompt intervention, may be the only action that prevents frank respiratory failure. Care must also be taken to evaluate for other conditions that may mimic acute exacerbations of COPD. evaluate for other conditions that may mimic acute exacerbations of COPD.
AECOPDs occur in clusters, not at random, as previously thought, according to an analysis by Hurst et al. Their study showed that patients with an AECOPD are at an increased risk of another attack in the 8 weeks following the initial episode. Close follow-up during this “brittle” period may lead to earlier treatment and better clinical outcomes.
A stepwise approach to drug therapy is recommended that takes into consideration the causes and complications related to the exacerbation, the degree of reversible bronchospasm, recent drug use, and contraindications to treatment. Sedation and pain management must be provided to ensure patient comfort and safety, despite a potential for respiratory depression.
Assisted ventilation
Progressive airflow obstruction may impair oxygenation and/or ventilation to the degree that the patient requires assisted ventilation. The general guidelines indicate that the ideal time to initiate ventilatory support are (1) when patients have experienced progressive worsening of respiratory acidosis and/or altered mental status and (2) when clinically significant hypoxemia exists despite supplemental oxygen.
Patients may be treated with noninvasive mask ventilation or with translaryngeal intubation and mechanical ventilation.
Bullectomy
The bullae in patients with emphysema generally range from 1-4 cm in diameter; on occasion, bullae can occupy more than 33% of the hemithorax (ie, giant bullae). Giant bullae may compress adjacent lung tissue, thereby reducing blood flow and ventilation to healthier tissue.
Removal of these bullae, a standard treatment in selected patients for many years, may result in the expansion of compressed lung tissue and improved function. Patients who are symptomatic and have an FEV1 of less than 50% of the predicted value have a better outcome after bullectomy.
Bullectomy is performed through a midline sternotomy or a lateral incision, or by video-assisted thoracoscopy. Postoperative bronchopleural air leak is the major potential complication.
Lung Volume Reduction Surgery
Nearly 40 years ago, Brantigan et al first reported resectional surgery for diffuse emphysema in 33 patients. They resected 20-30% of each lung that appeared most diseased. The investigators hypothesized that removal of a portion of the emphysematous lung would increase radial traction on the airways in the remaining lung, thereby reducing symptoms by improving expiratory airflow and mechanical function. The ICSI 2011 COPD guidelines state that lung reduction surgery may be an option for patients with severe symptoms that are not responding to maximal medical therapy.
Lung volume reduction surgery is carried out using a midline sternotomy with stapling of the lung margins. Surgeons generally resect 20-30% of each lung from the upper zones. The lung volume reduction procedure has a mortality rate of 0-18%. Several complications, including pneumonia and prolonged air leaks, have been observed.
Several studies, including the large, multicenter National Emphysema Treatment Trial (NETT), have demonstrated significant benefit in spirometry, exercise tolerance, dyspnea, health-related quality of life, and mortality in selected patients after LVRS.
Those who benefit most are patients with heterogeneous (upper lobe) disease and a low exercise capacity despite optimal medical therapy and cardiopulmonary rehabilitation. Patients with an FEV1 of less than 20% of predicted and either homogenous disease or DLCO (diffusing capacity of lung for carbon monoxide) of less than 20% of predicted are considered high risk for this procedure.
Lung Transplantation
Lung transplantation is performed only at select tertiary care centers around the world. Patients with COPD are the largest single category of patients who undergo the procedure.
When evaluating a potential candidate, several factors need be taken into account, including symptomatology, comorbid conditions, and projected survival without transplantation (eg, BODE index >5). Generally speaking, most centers set an age limit of 65 years.
The mean survival after lung transplantation is 5 years. The survival at 1 year is 80-90%. Whether this procedure has any effect on the survival of patients with COPD is controversial; the main purpose of lung transplantation is to improve symptomatology and quality of life.
Long-term Monitoring
Follow-up
Disposition after an AECOPD depends on the clinical picture for each patient more than on any single laboratory value or test. In general, the longer the exacerbation, the more airway edema and debris are present. Nearly all discharged patients should receive a short steroid burst and an increase in the frequency of inhaler therapy. Close follow-up should be arranged with the patient's regular care provider. Other therapies should be considered on a case-by-case basis.
Additional follow-up recommendations are as follows:
- Patients with severe or unstable disease should be seen monthly
- When their condition is stable, patients may be seen biannually
- Check theophylline level with each dose adjustment, when interacting medications are added, and routinely every 6-12 months
- For patients on home oxygen, check arterial blood gases (ABGs) yearly or with any change in condition
- Monitor oxygen saturation more frequently than ABGs
Pulmonary rehabilitation
Many patients with COPD are unable to enjoy life to the fullest because of shortness of breath, physical limitations, and inactivity. Pulmonary rehabilitation encompasses an array of therapeutic modalities designed to improve the patient's quality of life by decreasing airflow limitation, preventing secondary medical complications, and alleviating respiratory symptoms. The 3 major goals of the comprehensive management of COPD are the following:
- Lessen airflow limitation
- Prevent and treat secondary medical complications (eg, hypoxemia, infection)
- Decrease respiratory symptoms and improve quality of life
Successful implementation of a pulmonary rehabilitation program usually requires a team approach, with individual components provided by healthcare professionals who have experience in managing COPD (eg, physician, dietitian, nurse, respiratory therapist, exercise physiologist, physical therapist, occupational therapist, recreational therapist, cardiorespiratory technician, pharmacist, psychosocial professionals). This multidisciplinary approach emphasizes the following:
- Patient and family education
- Smoking cessation
- Medical management (including oxygen and immunization)
- Respiratory and chest physiotherapy
- Physical therapy with bronchopulmonary hygiene, exercise, and vocational rehabilitation
- Psychosocial support
As a result of rehabilitation, improvements have been shown in objective measures of patients’ quality of life, well-being, and health status, including reduction in respiratory symptoms, increases in exercise tolerance and functional activities (eg, walking), reduction in anxiety and depression, and increases in feelings of control and self-esteem.
An observational study has shown that pulmonary rehabilitation also improves the BODE index score in patients with COPD and is associated with better outcomes. Quality of life improvements after pulmonary rehabilitation can also be measured using the COPD Assessment Test (CAT), an 8-question patient-completed instrument. In addition, pulmonary rehabilitation results in substantial savings in health care costs by reducing hospitalizations and the use of medical resources.
Pulmonary rehabilitation programs usually are conducted in an outpatient setting. A rehabilitation program may include a number of components and should be tailored to the needs of the individual patient. Provide all patients who complete the program with guidelines for continuing at home.
Education is key to comprehensive pulmonary rehabilitation. The educational component prepares the patient and family to be actively involved in providing care. This reliance on patients to assume charge of their care is known as collaborative self-management.
Exercise training is a mandatory component of pulmonary rehabilitation. Patients with COPD should perform aerobic lower extremity endurance exercises regularly to enhance performance of daily activities and reduce dyspnea. Upper extremity exercise training improves dyspnea and allows increased activities of daily living requiring the use of upper extremities.
Breathing retraining techniques (eg, diaphragmatic, pursed lip breathing) may improve the ventilatory pattern and prevent dynamic airway compression.
 Pulmonary rehabilitation.
Pulmonary rehabilitation.Special concerns
Many commercial airplanes fly at altitudes of 30,000-40,000 feet. However, the cabin is pressurized to an altitude of 5000-8000 feet. At these altitudes, atmospheric partial pressure of oxygen (PO2) is 132-109 mm Hg, compared with 159 mm Hg at sea level.
Acute reduction in PO2 stimulates peripheral chemoreceptors, which results in hyperventilation. When determining whether or not a COPD patient can safely fly, the clinician should first use a prediction equation to determine whether the patient will become hypoxemic at high altitudes. A prediction equation used to estimate PaO2 at 8000 feet (2440 m) is as follows:
PaO2 = 22.8 - 2.74X + 0.68Y
(X = altitude; Y = arterial PO2 at sea level)
A predicted PaO2 of 50 mm Hg or less at an altitude of 8000 feet is an indication for supplemental oxygen. Arrange supplemental oxygen prior to the flight directly through the airline or through the airline agent (at an extra expense). If there is any question regarding the calculation, many pulmonary physiology labs can also perform altitude simulation tests to confirm or refute the need for in-flight oxygen.
Patients with COPD may develop substantial decreases in nocturnal PaO2 during all phases of sleep, but particularly during the rapid eye movement phase. These episodes are associated initially with a rise in pulmonary arterial pressures and a disturbance in sleep architecture, but they may develop into pulmonary arterial hypertension and cor pulmonale if hypoxemia remains untreated.
Prescribe oxygen for patients who have daytime PaO2 greater than 60 mm Hg but who demonstrate substantial nocturnal hypoxemia.
End-of-Life Care
COPD is a chronic disease that is preventable and treatable but largely incurable. Given the progressive nature of the disease, as well as the morbidity and mortality associated with it, clinicians should always include end-of-life care discussions in their visits with patients. These discussions should focus on palliative efforts to improve quality of life, as well as assistance with advanced directives, advanced care planning, and referrals for hospice and home care when needed.
Medication Summary
Oral and inhaled medications are used for patients with stable chronic obstructive pulmonary disease (COPD) to reduce dyspnea, improve exercise tolerance, and prevent complications. Most of the medications used in COPD treatment are directed at the following 4 potentially reversible mechanisms of airflow limitation:
- Bronchial smooth muscle contraction
- Bronchial mucosal congestion and edema
- Airway inflammation
- Increased airway secretions
Bronchodilators act to decrease muscle tone in small and large airways in the lungs, thereby increasing ventilation. The category includes subcutaneous medications, beta-adrenergics, methylxanthines, and anticholinergics.
Additionally, opioids have been shown in multiple studies to relieve dyspnea, particularly near the end of life. Dosage is very patient specific. Currow et al used a low, once-daily dose of sustained-release morphine for chronic refractory dyspnea.
Beta2-Adrenergic Agonists, Short-Acting
Class Summary
Beta2 -agonists activate specific B2 -adrenergic receptors on the surface of smooth muscle cells, which increases intracellular cyclic adenosine monophosphate (cAMP) and smooth muscle relaxation. Beta2 -agonists produce less bronchodilatation in COPD than in asthma. Patients use beta2 -agonists primarily for relief of symptoms of COPD. In patients with mild, intermittent symptoms, short-acting beta2 -agonists is recommended for symptomatic relief.
Beta2-Adrenergic Agonists, Long-Acting
Class Summary
Beta2 -agonist bronchodilators activate specific beta2 -adrenergic receptors on the surface of smooth muscle cells, which increases intracellular cyclic adenosine monophosphate (cAMP) and smooth muscle relaxation. In patients with more persistent symptoms, a long-acting beta agonist should be used. Long-acting beta agonists have been shown to increase exercise endurance, prevent nocturnal dyspnea, and improve quality of life. Long-acting beta-agonists include salmeterol, formoterol, arformoterol, and indacaterol. They all require twice-daily dosing, except for indacaterol and olodaterol, which are administered once daily.
Anticholinergics, Respiratory
Class Summary
Anticholinergic drugs compete with acetylcholine for postganglionic muscarinic receptors, thereby inhibiting cholinergically mediated bronchomotor tone, resulting in bronchodilatation. They block vagally mediated reflex arcs that cause bronchoconstriction. Clinical benefit is gained through a decrease in exercise-induced dynamic hyperinflation. These agents are poorly absorbed systemically and are relatively safe. Reported adverse effects include dry mouth, metallic taste, and prostatic symptoms.
Xanthine Derivative
Class Summary
Xanthine derivatives such as theophylline relax the smooth muscles of the bronchi and pulmonary blood vessels. Inhibition of phosphodiesterase by these agents causes an increase in cyclic adenosine monophosphate (cAMP), causing the relaxation of bronchial smooth muscles.
Corticosteroids, Inhalant
Class Summary
In acute exacerbations, steroids improve symptoms and lung function. Inhaled corticosteroids provide a more direct route of administration to the airways and, similar to other inhaled agents, are only minimally absorbed. Inhaled steroids have fewer adverse effects than do oral agents, although they improve expiratory flows less effectively, even at high doses. These agents may be beneficial in slowing the rate of progression in a subset of patients with COPD who have rapid decline.
Corticosteroids, Oral
Class Summary
The use of oral steroids in the treatment of acute exacerbations is widely accepted and recommended, given their high efficacy. Note that oral steroids are not as effective in treating COPD exacerbations as they are in treating bronchial asthma exacerbations.
Beta-Adrenergic Agonist and Anticholinergic Agent Combinations
Class Summary
These agents combine the benefits of the rapid onset of a beta-adrenergic agonist with the prolonged action of an anticholinergic agent.
Beta2-Adrenergic Agonist and Corticosteroid Combinations
Class Summary
Combination therapy is recommended when COPD patients are uncontrolled with bronchodilator monotherapy. Agents that use a long-acting beta agonist and an inhaled corticosteroid are commonly used in asthma and COPD and show increased clinical benefits.
Antibiotics
Class Summary
In patients with COPD, chronic infection or colonization of the lower airways is common from S pneumoniae, H influenzae, and M catarrhalis. In patients with chronic severe airway obstruction, P aeruginosa infection may also be prevalent. The use of antibiotics for the treatment of acute exacerbations is well supported.
Smoking Cessation Therapies
Class Summary
Smoking cessation continues to be the most important therapeutic intervention for COPD. Supervised use of pharmacologic agents is an important adjunct to self-help and group smoking cessation programs. Nicotine replacement therapies after smoking cessation reduce withdrawal symptoms.
 Posted in
Posted in
ReplyDeleteFor people suffering from COPD, it is important for them to know that they are not alone. I was also a victim.
I had experienced shortness of breath, coughing, recurring chest infections and bronchitis. But I didn’t realize that I had COPD until I went to my doctor and was diagnosed with COPD. The first thing I did was get myself informed. Having COPD hasn’t slowed me down. Even though I had COPD I still played golf and involved myself in different excercise though I started smoking at 19 years of age I smoked almost a pack a day. The doctor had told me to quit smoking, it was frightening and frustrating, I thought it was to avoid stress. I learned about Dr. Lance Herbal Medicine from a friend. Now my life has turned around for good because I consider myself most fortunate.
There are so many people out there who have COPD and don’t realize it.
If you have COPD, many things are available to help you live a full, comfortable life don’t be ashamed of it.
I can’t speak for everyone. I can guarantee that this Herbal Medicine will work for you and I suggest you try it. It has done wonders for me. contact him on lancejustin54@gmail.com for more information and advice.
After having a persistent cough for over a year, I was diagnosed with COPD
Deletein March 2015. In 2016 my COPD got worse to the point where not only do I
have trouble sleeping at night, I also struggle to get air into my lungs. I
read in a health forum of a herbal centre (native health clinic) who have successful treatment to COPD/Emphysema, i immediately
contacted the herbal centre via their website and purchased the COPD herbal
remedy, I used the remedy for 2 weeks, all my symptoms were reversed, i did
another test for confirmation, i was declared COPD free. email (
nativehealthclinic@gmail.com) or WhatsApp/Call him on +2348140073965
ReplyDeleteFor people suffering from COPD, it is important for them to know that they are not alone. I was also a victim.
I had experienced shortness of breath, coughing, recurring chest infections and bronchitis. But I didn’t realize that I had COPD until I went to my doctor and was diagnosed with COPD. The first thing I did was get myself informed. Having COPD hasn’t slowed me down. Even though I had COPD I still played golf and involved myself in different excercise though I started smoking at 19 years of age I smoked almost a pack a day. The doctor had told me to quit smoking, it was frightening and frustrating, I thought it was to avoid stress. I learned about Dr. Lance Herbal Medicine from a friend. Now my life has turned around for good because I consider myself most fortunate.
There are so many people out there who have COPD and don’t realize it.
If you have COPD, many things are available to help you live a full, comfortable life don’t be ashamed of it.
I can’t speak for everyone. I can guarantee that this Herbal Medicine will work for you and I suggest you try it. It has done wonders for me. contact him on lancejustin54@gmail.com for more information and advice.
ReplyDeleteFor people suffering from COPD, it is important for them to know that they are not alone. I was also a victim.
I had experienced shortness of breath, coughing, recurring chest infections and bronchitis. But I didn’t realize that I had COPD until I went to my doctor and was diagnosed with COPD. The first thing I did was get myself informed. Having COPD hasn’t slowed me down. Even though I had COPD I still played golf and involved myself in different excercise though I started smoking at 19 years of age I smoked almost a pack a day. The doctor had told me to quit smoking, it was frightening and frustrating, I thought it was to avoid stress. I learned about Dr. Lance Herbal Medicine from a friend. Now my life has turned around for good because I consider myself most fortunate.
There are so many people out there who have COPD and don’t realize it.
If you have COPD, many things are available to help you live a full, comfortable life don’t be ashamed of it.
I can’t speak for everyone. I can guarantee that this Herbal Medicine will work for you and I suggest you try it. It has done wonders for me. contact him on lancejustin54@gmail.com for more information and advice.
HOW I CURED MY CHRONIC BRONCHITIS THROUGH HERBS
ReplyDeleteThis may help those going through what I went through. I worked a long time for a Pesticide Company, and was diagnosed of Chronic Bronchitis. I used all prescribed medications and steroids yet, my condition got more complicated. The more I take antibiotics and kenalog injection, the worst the Bronchitis became. It got to a point the wheezing was just too much and I had constant fever and other complications which resulted from the drugs I was taking which couldn't provide a cure. I got feed up and went in search for a natural cure. At first, I thought I was the only one in the world was had Chronic Bronchitis, until I read a testimony of someone who got cured through herbal remedy without side effects. I contacted the doctor, explained my case and I got herbal medication which I used. Within one month of use, I was free from mucus and phlegm. In case you have someone suffering from bronchitis, you may contact Dr. Scott where I got my natural herbal cure via drevanscott@gmail.com
I want to use this medium to appreciate the admin of this page for allowing me to share my story.I believe that this will help others going through what i went through over the years to find a cure like i did. i was diagonosed of COPD which i suffered for so many years, despite the different english medications i took in order to find a cure, it didn't work. i started having complications resulting from those english medications i was taking over the years. as a result of these complications from my drugs, i went in search for a natural cure where i saw a testimony of someone who suffered the same sickness i was going through and the person got his cure through herbal medication, then, i followed the email he shared and i contacted the doctor, i got my cure as well, incase you are going through same sickness, you may contact the doctor for more information through his email: drallenchase@gmail.com
ReplyDeletei want to use this medium to appreciate the admin of this page for allowing me to share my story.i believe that this will help others going through what i went through over the years to find a cure like i did. i was diagonosed of COPD which i suffered for so many years, despite the different english medications i took in order to find a cure, it didn't work. i started having complications resulting from those english medications i was taking over the years. as a result of these complications from my drugs, i went in search for a natural cure where i saw a testimony of someone who suffered the same sickness i was going through and the person got his cure through herbal medication, then, i followed the email he shared and i contacted the doctor, i got my cure as well, incase you are going through same sickness, you may contact the doctor through his email: drallenchase@gmail.com
ReplyDeleteBronchiectasis is a pulmonary condition that appears when there is permanent enlargement of parts of the airways of the lung. The most common symptoms are suppurative infections and severe cough. Here is a complete Bronchiectasis Natural Treatment that has healed so lots of people.
ReplyDeleteI have been diagnosed with COPD (chronic obstructive pulmonary disease) and my doctor has given me Seebri Breezhaler, it's an inhalation powder 44 micrograms. I take it once a day in the morning. It's a great help to breathing, it's a new medicine on test, 10 out of 10 from me! But still yet i was told it has no cure for it. I was fed up to nearly take my life until my son saw a post of a lady who testify that there's a cure for copd and she was diagnosed with this disease for 8 years before she came arrow a website of an Africa clinic. Which provide natural herbal herbs to cure copd and she purchase it through online. My son purchase their copd herbal remedy on my behalf and give it to me to use with the instructions given on how to apply it, when i applied it as instructed i was totally cured of this deadly disease within 12 weeks of usage. I advise whosoever reading my testimony should visit www.solutionhealthherbalclinic.com and seek for your solution, You also can email at solutionsherbalclinic@gmail.com.
ReplyDeleteI had COPD for 9 years. My first symptoms were dry cough, chest tightness and shortness of breath. My first chest x-ray only showed bronchitis. Finally I went to a pulmonologist and was diagnosed with COPD.i have used all the medication yet they don’t work, last year December I was told by a formal emphysema patient to use totalcureherbalfoundation@gmail.com herbal treatment which I really did,i was surprise the herbal products effectively get rid of my COPD totally. When you get where you cannot breathe it may be too late. Good luck to each and every one that will be trying their herbal treatment .
ReplyDeleteMy father was born with asthma in his later years he suffered from COPD and emphysema. His doctor told him if he get the flu or really sick that could be the end. He have been nearly gone many times, why is he still here I am not sure maybe God. It is a hard life to live and I always hope that someday someone will figure out a cure not until my family found www. totalcureherbsfoundation. com remedies that gradually cure and relief this lung conditions after several weeks of the dosage . I always think it is not taken as seriously as it should be ever since my father use the natural herbal medication from that company his condition and the breathing system and all that has been extremely reversed to normal .
ReplyDeleteI started on COPD Herbal treatment from Ultimate Health Home, the treatment worked incredibly for my lungs condition. I used the herbal treatment for almost 4 months, it reversed my COPD. My severe shortness of breath, dry cough, chest tightness gradually disappeared. Reach Ultimate Health Home via their email at ultimatehealthhome@gmail.com . I can breath much better and It feels comfortable!
ReplyDeleteRhonda S.’s COPD made her feel short of breath and like she was constantly dragging. While her inhalers helped some, she just didn’t feel like herself anymore.
ReplyDeleteAfter having life-threatening pneumonia, she knew something had to change. A friend of hers mentioned multivitamin herbal formula restoration treatment, so Rhonda did
some research and decided to receive treatment at the multivitamin herbal cure. “I started to feel better almost right away,” Rhonda said.
And, along with feeling better, she began to do things she couldn’t do before treatment. Now, Rhonda can take showers, work in her flower garden, and she enjoys having more energy. It’s with a great deal of hope, Rhonda says, “I feel more like myself.”
Like Rhonda, you can breathe easier and bring normal life back within reach. If you or someone you love has a chronic lung disease and would like more information, contact us today by calling (+1 (956) 758-7882 to visit their website multivitamincare .org