 RSS Feed
RSS Feed Twitter
Twitter


 Sunday, March 29, 2015
Sunday, March 29, 2015
 Unknown
Unknown
Bell palsy, also termed idiopathic facial paralysis (IFP), is the most common cause of unilateral facial paralysis and the most common cause of facial paralysis worldwide. It is one of the most common neurologic disorders of the cranial nerves (see the image below). In the great majority of cases, Bell palsy gradually resolves over time, and its cause is unknown.
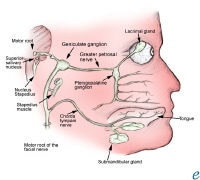 The facial nerve.
The facial nerve.Essential update: New Bell palsy guidelines issued by The American Academy of Otolaryngology—Head and Neck Surgery Foundation
The American Academy of Otolaryngology—Head and Neck Surgery Foundation has issued updated guidelines for the diagnosis and management of Bell palsy that recommend the use of corticosteroids within 72 hours after the onset of symptoms in patients 16 years of age and older. Antiviral agents (eg, acyclovir, valacyclovir) may be considered if a viral etiology is suspected, but only in combination with corticosteroids.
Additional recommendations include the following :
- Patients with acute-onset unilateral facial paralysis should be assessed to exclude other possible identifiable causes (eg, herpes zoster, Lyme disease, sarcoidosis)
- Diagnostic imaging and routine lab testing are not recommended for patients with new-onset disease
- Electrodiagnostic testing is not recommended in patients with incomplete facial paralysis; however, it may be offered to those patients with complete facial paralysis
- If there is impaired eye closure, appropriate eye protection should be implemented
- Referral to a facial nerve specialist should occur in cases of new or worsening neurologic symptoms, developing ocular symptoms, or incomplete facial recovery after 3 months
Signs and symptoms
Signs and symptoms of Bell palsy include the following:
- Acute onset of unilateral upper and lower facial paralysis (over a 48-hr period)
- Posterior auricular pain
- Decreased tearing
- Hyperacusis
- Taste disturbances
- Otalgia
- Weakness of the facial muscles
- Poor eyelid closure
- Aching of the ear or mastoid
- Tingling or numbness of the cheek/mouth
- Epiphora
- Ocular pain
- Blurred vision
- Flattening of forehead and nasolabial fold on the side affected by palsy
- When patient raises eyebrows, palsy-affected side of forehead remains flat
- When patient smiles, face becomes distorted and lateralizes to side opposite the palsy
Diagnosis
Examination for Bell palsy includes the following:
- Otologic examination: Pneumatic otoscopy and tuning fork examination, particularly if evidence of acute or chronic otitis media
- Ocular examination: Patient often unable to completely close eye on affected side
- Oral examination: Taste and salivation often affected
- Neurologic examination: All cranial nerves, sensory and motor testing, cerebellar testing
Grading
The grading system developed by House and Brackmann categorizes Bell palsy on a scale of I to VI, as follows:
Grade I: normal facial function
Grade II: mild dysfunction
Grade III: moderate dysfunction
Grade IV: moderately severe dysfunction
Grade V: severe dysfunction
Grade VI: total paralysis
Testing
Although there are no specific diagnostic tests for Bell palsy, the following may be useful for identifying or excluding other disorders:
- Rapid plasma reagin and/or venereal disease research laboratory test or fluorescent treponemal antibody absorption test
- HIV screening by enzyme-linked immunosorbent assay and/or Western blot
- Complete blood count
- Erythrocyte sedimentation rate
- Thyroid function
- Serum glucose
- CSF analysis
- Blood glucose
- Hemoglobin A1c
- Antineutrophil cytoplasmic antibody levels
- Salivary flow
- Schirmer blotting test
- Nerve excitability test
- Computed tomography
- Magnetic resonance imaging
Management
Goals of treatment: (1) improve facial nerve (seventh cranial nerve) function; (2) reduce neuronal damage; (3) prevent complications from corneal exposure
Treatment includes the following:
- Corticosteroid therapy (prednisone)
- Antiviral agents
- Eye care: Topical ocular lubrication is usually sufficient in most cases to prevent corneal drying, abrasion, and ulcers
Surgical options
Surgical treatment options include the following:
- Facial nerve decompression
- Subocularis oculi fat lift
- Implantable devices (eg, gold weights) placed into the eyelid
- Tarsorrhaphy
- Transposition of the temporalis muscle
- Facial nerve grafting
- Direct brow lift
Background
Bell palsy, more appropriately termed idiopathic facial paralysis (IFP), is the most common cause of unilateral facial paralysis. Bell palsy is an acute, unilateral, peripheral, lower-motor-neuron facial nerve paralysis that gradually resolves over time in 80-90% of cases.
Controversy surrounds the etiology and treatment of Bell palsy. The cause of Bell palsy remains unknown, though the disorder appears to be a polyneuritis with possible viral, inflammatory, autoimmune, and ischemic etiologies. Increasing evidence implicates herpes simplex type I and herpes zoster virus reactivation from cranial-nerve ganglia.
Bell palsy is one of the most common neurologic disorders affecting the cranial nerves, and it is the most common cause of facial paralysis worldwide. It is thought to account for approximately 60-75% of cases of acute unilateral facial paralysis. Bell palsy is more common in adults, in people with diabetes, and in pregnant women. (See Epidemiology.)
Diagnosis
Determining whether facial nerve paralysis is peripheral or central is a key step in the diagnosis. A lesion involving the central motor neurons above the level of the facial nucleus in the pons causes weakness of the lower face alone. Thorough history taking and examination, including the ears, nose, throat, and cranial nerves, must be performed. (See Presentation.)
The minimum diagnostic criteria include paralysis or paresis of all muscle groups on one side of the face, sudden onset, and absence of central nervous system (CNS) disease. Note that the diagnosis of IFP can be made only after other causes of acute peripheral palsy have been excluded.
If the clinical findings are doubtful or if paralysis lasts longer than 6-8 weeks, further investigations, including gadolinium-enhanced magnetic resonance imaging (MRI) of the temporal bones and pons, should be considered. Electrodiagnostic tests (eg, stapedius reflex test, evoked facial nerve electromyography [EMG], audiography) may help to improve the accuracy of prognosis in difficult cases.
Treatment
Treatment of Bell palsy should be conservative and guided by the severity and probable prognosis in each particular case. Studies have shown the benefit of high-dose corticosteroids for acute cases. Although antiviral treatment has also come into use, evidence is now available indicating that it may not be beneficial.
Topical ocular therapy is useful in most cases, with the exception of those in which the condition is severe or prolonged. In these cases, surgical management is best. Several procedures are aimed at protecting the cornea from exposure and achieving facial symmetry. These procedures reduce the need for constant use of lubrication drops or ointments, may improve cosmesis, and may be needed to preserve vision on the affected side. (See Treatment.)
Patient education
To prevent corneal abrasions, patients should be instructed about eye care. They also should be encouraged to do facial muscle exercises using passive range of motion, as well as actively close their eyes and smile.
Anatomy
In 1550, Fallopius noted the narrow foramen in the temporal bone through which a part of the seventh cranial nerve (facial nerve) passes; this feature is now sometimes called the fallopian canal or the facial canal. In 1828, Charles Bell made the distinction between the fifth and seventh cranial nerves; he noted that the seventh nerve was involved mainly in the motor function of the face and that the fifth nerve primarily conducted sensation from the face.
The facial nerve contains parasympathetic fibers to the nose, palate, and lacrimal glands. Its course is tortuous, both centrally and peripherally. The facial nerve travels a 30-mm intraosseous course through the internal auditory canal (with the eighth cranial nerve) and through the internal fallopian canal in the petrous temporal bone. This bony confinement limits the amount that the nerve can swell before it becomes compressed.
The nucleus of the facial nerve lies within the reticular formation of the pons, adjacent to the fourth ventricle. The facial nerve roots include fibers from the motor, solitary, and salivatory nuclei. The preganglionic parasympathetic fibers that originate in the salivatory nucleus join the fibers from nucleus solitarius to form the nervus intermedius.
The nervus intermedius is composed of sensory fibers from the tongue, mucosa, and postauricular skin, as well as parasympathetic fibers to the salivary and lacrimal glands. These fibers then synapse with the submandibular ganglion, which has fibers that supply the sublingual and submandibular glands. The fibers from the nervus intermedius also supply the pterygopalatine ganglion, which has parasympathetic fibers that supply the nose, palate, and lacrimal glands.
The fibers of the facial nerve then course around the sixth cranial nerve nucleus and exit the pons at the cerebellopontine angle. The fibers go through the internal auditory canal along with the vestibular portion of the eighth cranial nerve.
The facial nerve passes through the stylomastoid foramen in the skull and terminates into the zygomatic, buccal, mandibular, and cervical branches. These nerves serve the muscles of facial expression, which include the frontalis, orbicularis oculi, orbicularis oris, buccinator, and platysma muscles. Other muscles innervated by the facial nerve include the stapedius, stylohyoid, posterior belly of the digastric, occipitalis, and anterior and posterior auricular muscles. All muscles innervated by the facial nerve are derived from the second branchial arch. See the images below.
The facial nerve.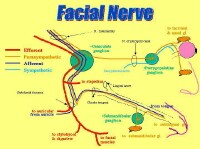 The facial nerve.
The facial nerve.Pathophysiology
The precise pathophysiology of Bell palsy remains an area of debate. The facial nerve courses through a portion of the temporal bone commonly referred to as the facial canal. A popular theory proposes that edema and ischemia result in compression of the facial nerve within this bony canal. The cause of the edema and ischemia has not yet been established. This compression has been seen in MRI scans with facial nerve enhancement.
The first portion of the facial canal, the labyrinthine segment, is the narrowest; the meatal foramen in this segment has a diameter of only about 0.66 mm. This is the location that is thought to be the most common site of compression of the facial nerve in Bell palsy. Given the tight confines of the facial canal, it seems logical that inflammatory, demyelinating, ischemic, or compressive processes may impair neural conduction at this site.
Injury to the facial nerve in Bell palsy is peripheral to the nerve’s nucleus. The injury is thought to occur near, or at, the geniculate ganglion. If the lesion is proximal to the geniculate ganglion, the motor paralysis is accompanied by gustatory and autonomic abnormalities. Lesions between the geniculate ganglion and the origin of the chorda tympani produce the same effect, except that they spare lacrimation. If the lesion is at the stylomastoid foramen, it may result in facial paralysis only.
Etiology
Herpes simplex virus
In the past, situations that produced cold exposure (eg, chilly wind, cold air conditioning, or driving with the car window down) were considered to be the only triggers for Bell palsy. Several authors now believe, however, that the herpes simplex virus (HSV) is a common cause of Bell palsy, though a definitive causal relationship of HSV to Bell palsy may be difficult to prove because of the ubiquitous nature of HSV.
The hypothesis that HSV is the etiologic agent in Bell palsy holds that after causing primary infection on the lips (ie, cold sores), the virus travels up the axons of the sensory nerves and resides in the geniculate ganglion. At times of stress, the virus reactivates and causes local damage to the myelin.
This hypothesis was first suggested in 1972 by McCormick. Autopsy studies have since shown HSV in the geniculate ganglion of patients with Bell palsy. Murakami et al performed polymerase chain reaction (PCR) assay testing on the endoneural fluid of the facial nerve in patients who underwent surgery for Bell palsy and found HSV in 11 of 14 cases.
Additional support for a viral etiology was seen when intranasal, inactivated influenza vaccine was strongly linked to the development of Bell palsy. With those cases, however, it is not clear whether another component of the vaccine caused the paresis, which was then accompanied by a reactivation of HSV infection.
Additional causes
Besides HSV infection, possible etiologies for Bell palsy include other infections (eg, herpes zoster, Lyme disease, syphilis, Epstein-Barr viral infection, cytomegalovirus, human immunodeficiency virus [HIV], mycoplasma); inflammation alone; and microvascular disease (diabetes mellitus and hypertension). Bell palsy has also been known to follow recent upper respiratory infection (URI).
Bell palsy may be secondary to viral and/or autoimmune reactions that cause the facial nerve to demyelinate, resulting in unilateral facial paralysis.
A family history of Bell palsy has been reported in approximately 4% of cases. Inheritance in such cases may be autosomal dominant with low penetration; however, which predisposing factors are inherited is unclear. The family history may also be positive for other nerve, nerve root, or plexus disorders (eg, trigeminal neuralgia) in siblings. In addition, there are isolated reports of familial Bell palsy with neurologic deficits, including ophthalmoplegia and essential tremor. A rare form of familial Bell palsy has a predilection for juvenile females.
Because there is a strong environmental predisposition to Bell palsy, due to the common viral etiology, a positive family history may or may not indicate a true genetic etiology.
Epidemiology
In the United States, the annual incidence of Bell palsy is approximately 23 cases per 100,000 persons. Very few cases are observed during the summer months. Internationally, the highest incidence was found in a study in Seckori, Japan, in 1986, and the lowest incidence was found in Sweden in 1971. Most population studies generally show an annual incidence of 15-30 cases per 100,000 population.
Bell palsy is thought to account for approximately 60-75% of cases of acute unilateral facial paralysis, with the right side affected 63% of the time. It can also be recurrent, with a reported recurrence range of 4-14%.
Though bilateral simultaneous Bell palsy can develop, it is rare. It accounts for only 23% of bilateral facial paralysis and has an occurrence rate that is less than 1% of that for unilateral facial nerve palsy. The majority of patients with bilateral facial palsy have Guillain-Barré syndrome, sarcoidosis, Lyme disease, meningitis (neoplastic or infectious), or bilateral neurofibromas (in patients with neurofibromatosis type 2).
Persons with diabetes have a 29% higher risk of being affected by Bell palsy than do persons without diabetes. Thus, measuring blood glucose levels at the time of diagnosis of Bell palsy may detect undiagnosed diabetes. Diabetic patients are 30% more likely than nondiabetic patients to have only partial recovery; recurrence of Bell palsy is also more common among diabetic patients.
Bell palsy is also more common in people who are immunocompromised or in women with preeclampsia.
Sex- and age-related demographics
Bell palsy appears to affect the sexes equally. However, young women aged 10-19 years are more likely to be affected than are men in the same age group. Pregnant women have a 3.3 times higher risk of being affected by Bell palsy than do nonpregnant women; Bell palsy occurs most frequently in the third trimester.
In general, Bell palsy occurs more commonly in adults. A slightly higher predominance is observed in patients older than 65 years (59 cases per 100,000 people), and a lower incidence rate is observed in children younger than 13 years (13 cases per 100,000 people). The lowest incidence is found in persons younger than 10 years, and the highest incidence is in persons aged 60 years or older. Peak ages are between 20 and 40 years. The disease also occurs in elderly persons aged 70-80 years.
Prognosis
The natural course of Bell palsy varies from early complete recovery to substantial nerve injury with permanent sequelae (eg, persistent paralysis and synkinesis). Prognostically, patients fall into 3 groups:
- Group 1 - Complete recovery of facial motor function without sequelae
- Group 2 - Incomplete recovery of facial motor function, but with no cosmetic defects that are apparent to the untrained eye
- Group 3 - Permanent neurologic sequelae that are cosmetically and clinically apparent
Approximately 80-90% of patients with Bell palsy recover without noticeable disfigurement within 6 weeks to 3 months. Use of the Sunnybrook grading scale for facial nerve function at 1 month has been suggested as a means of predicting probability of recovery.
Most patients who suffer from Bell palsy have neurapraxia or local nerve conduction block. These patients are likely to have a prompt and complete recovery of the nerve. Patients with axonotmesis, with disruption of the axons, have a fairly good recovery, but it is usually not complete.
The risk factors thought to be associated with a poor outcome in patients with Bell palsy include (1) age greater than 60 years, (2) complete paralysis, and (3) decreased taste or salivary flow on the side of paralysis (usually 10-25% compared with the patient’s normal side). Other factors thought to be associated with poor outcome include pain in the posterior auricular area and decreased lacrimation.
Patients aged 60 years or older have an approximately 40% chance of complete recovery and have a higher rate of sequelae. Patients younger than 30 years have only a 10-15% chance of less than complete recovery and/or long-term sequelae.
The sooner the recovery, the less likely are the chances that sequelae will develop, as summarized below:
- If some restoration of function is noted within 3 weeks, then the recovery is most likely to be complete
- If the recovery begins between 3 weeks and 2 months, then the ultimate outcome is usually satisfactory
- If the recovery does not begin until 2-4 months from the onset, likelihood of permanent sequelae, including residual paresis and synkinesis, is higher
- If no recovery occurs by 4 months, then the patient is more likely to have sequelae from the disease, which include synkinesis, crocodile tears, and (rarely) hemifacial spasm
Bell palsy recurs in 4-14% of patients, with one source suggesting a recurrence rate of 7%. It may recur on the same or opposite side of the initial palsy. Recurrence usually is associated with a family history of recurrent Bell palsy. Higher recurrence rates among patients were reported in the past; however, many of these patients were found to have an underlying etiology for the recurrence, eliminating the diagnosis of Bell palsy, an idiopathic disease.
Patients with recurrent ipsilateral facial palsy should undergo MRI or high-resolution computed tomography (CT) scanning to rule out a neoplastic or inflammatory (eg, multiple sclerosis, sarcoidosis) cause of recurrence. Recurrent or bilateral disease should suggest myasthenia gravis.
Sequelae
Most patients with Bell palsy recover without any cosmetically obvious deformities. Approximately 30% of patients, however, experience long-term symptoms following the paralysis, and approximately 5% are left with an unacceptably high degree of sequelae. Bell palsy sequelae include incomplete motor regeneration, incomplete sensory regeneration, and aberrant reinnervation of the facial nerve.
Incomplete motor regeneration
The largest portion of the facial nerve is composed of efferent fibers that stimulate muscles of facial expression. Suboptimal regeneration of this portion results in paresis of all or some of these facial muscles. This manifests as (1) oral incompetence, (2) epiphora (excessive tearing), and (3) nasal obstruction.
Incomplete sensory regeneration
Dysgeusia or ageusia (impairment or loss of taste, respectively) may occur with incomplete regeneration of the chorda tympani. Incomplete regeneration of other afferent branches may result in dysesthesia (impairment of sensation or disagreeable sensation to normal stimuli).
Aberrant reinnervation of the facial nerve
During regeneration and repair of the facial nerve, some neural fibers may take an unusual course and connect to neighboring muscle fibers. This aberrant reconnection produces unusual neurologic pathways. When voluntary movements are initiated, they are accompanied by involuntary movements (eg, eye closure associated with lip pursing or mouth grimacing that occurs during blinking of the eye). The condition in which involuntary movements accompany voluntary movements is termed synkinesis.
History
The diagnosis of Bell palsy must be made on the basis of a thorough history and physical examination, as well as the use of diagnostic testing when necessary. Bell palsy is a diagnosis of exclusion. Clinical features of the disorder that may help to distinguish it from other causes of facial paralysis include the sudden onset of unilateral facial paralysis and the absence of signs and symptoms of CNS, ear, and cerebellopontine angle disease.
Symptoms of Bell palsy include the following:
- Acute onset of unilateral upper and lower facial paralysis (over a 48-h period)
- Posterior auricular pain
- Decreased tearing
- Hyperacusis
- Taste disturbances
- Otalgia
Early symptoms include the following:
- Weakness of the facial muscles
- Poor eyelid closure
- Aching of the ear or mastoid (60%)
- Alteration of taste (57%)
- Hyperacusis (30%)
- Tingling or numbness of the cheek/mouth
- Epiphora
- Ocular pain
- Blurred vision
Onset
The onset of Bell palsy is typically sudden, and symptoms tend to peak in less than 48 hours. This sudden onset can be frightening for patients, who often fear they have had a stroke or have a tumor and that the distortion of their facial appearance will be permanent.
Because the condition appears so rapidly, patients with Bell palsy frequently present to the emergency department (ED) before seeing any other health care professional. More people first notice paresis in the morning. Because the symptoms require several hours to become evident, most cases of paresis likely begin during sleep.
Facial paralysis
The paralysis must include the forehead and lower aspect of the face. The patient may report the inability to close the eye or smile on the affected side. He or she also may report increased salivation on the side of the paralysis. If the paralysis involves only the lower portion of the face, a central cause should be suspected (ie, supranuclear). If the patient complains of contralateral weakness or diplopia in conjunction with the supranuclear facial palsy, a stroke or intracerebral lesion should be strongly suspected.
If a patient has gradual onset of facial paralysis, weakness of the contralateral side, or a history of trauma or infection, other causes of facial paralysis must be strongly considered. Progression of the paresis is possible, but it usually does not progress beyond 7-10 days. A progression beyond this point suggests a different diagnosis. Patients who have bilateral facial palsy must be evaluated for Guillain-Barré syndrome, Lyme disease, and meningitis.
Many patients report numbness on the side of the paralysis. Some authors believe that this is secondary to involvement of the trigeminal nerve, whereas other authors argue that this symptom is probably from lack of mobility of the facial muscles and not lack of sensation.
Ocular manifestations
Early ocular complications include the following:
- Lagophthalmos (inability to close the eye completely)
- Paralytic ectropion of the lower lid
- Corneal exposure
- Brow droop
- Upper eyelid retraction
- Decreased tear output/poor tear distribution
- Loss of the nasolabial fold
- Corneal erosion, infection, and ulceration (rare)
Late ocular manifestations include the following:
- Mild, generalized mass contracture of the facial muscles, rendering the affected palpebral fissure narrower than the opposite one (after several months)
- Aberrant regeneration of the facial nerve with motor synkinesis
- Reversed jaw winking (ie, contracture of the facial muscles with twitching of the corner of the mouth or dimpling of the chin occurring simultaneously with each blink)
- Autonomic synkinesis (ie, crocodile tears—tearing with chewing)
- Permanent, disfiguring facial paralysis (rare)
Two thirds of patients complain about tear flow. This results from the reduced function of the orbicularis oculi in transporting the tears. Fewer tears arrive at the lacrimal sac, and overflow occurs. The production of tears is not accelerated.
Posterior auricular pain
Half of the patients affected with Bell palsy may complain of posterior auricular pain. The pain frequently occurs simultaneously with the paresis, but pain precedes the paresis by 2-3 days in about 25% of patients. Ask the patient if he or she has experienced trauma, which may account for the pain and facial paralysis.
One third of patients may experience hyperacusis in the ear ipsilateral to the paralysis, which is secondary to weakness of the stapedius muscle.
Taste disorders
While only one third of patients report taste disorders, 80% of patients show a reduced sense of taste. Patients may fail to note reduced taste, because of normal sensation in the uninvolved side of the tongue. Early recovery of the sense of taste suggests that the patient will experience a complete recovery.
Facial spasm
Facial spasm, a very rare complication of Bell palsy, occurs as tonic contraction of 1 side of the face. Spasms are more likely to occur during times of stress or fatigue and may be present during sleep. This condition may occur secondary to compression of the root of the seventh nerve by an aberrant blood vessel, tumor, or demyelination of the nerve root.
Facial spasm occurs most commonly in patients in the fifth and sixth decades of life. Sometimes the etiology is not found. The presence of progressive facial hemispasm with other cranial nerve findings indicates the possibility of a brainstem lesion.
Synkinesis is an abnormal contracture of the facial muscles while smiling or closing the eyes. It may be mild and result in slight movement of the mouth or chin when the patient blinks or in eye closure with smiling. Crocodile tears can be observed; patients shed tears while they eat.
Cranial neuropathies
Some believe that other cranial neuropathies may also be present in Bell palsy; however, this is not uniformly accepted. The symptoms in question include the following:
- Hyperesthesia or dysesthesia of the glossopharyngeal or trigeminal nerves
- Dysfunction of the vestibular nerve
- Hyperesthesia of the cervical sensory nerves
- Vagal or trigeminal motor weakness
Physical Examination
Weakness and/or paralysis from involvement of the facial nerve affects the entire face (upper and lower) on the affected side. A careful examination of the head, ears, eyes, nose, and throat must be carried out in all patients with facial paralysis. Time must also be taken to examine the patient’s skin for signs of squamous cell carcinoma, which can invade the facial nerve, and parotid gland disease.
Focus attention on the voluntary movement of the upper part of the face on the affected side; in supranuclear lesions, such as occur in a cortical stroke (upper motor neuron; above the facial nucleus in the pons), the upper third of the face is spared in the majority of cases, while the lower two thirds are paralyzed. The orbicularis, frontalis, and corrugator muscles are innervated bilaterally at the level of the brainstem, which explains the pattern of facial paralysis in these cases.
Initial inspection of the patient demonstrates flattening of the forehead and nasolabial fold on the side affected by the palsy. When the patient is asked to raise his or her eyebrows, the side of the forehead with the palsy will remain flat. When the patient is asked to smile, the face will become distorted and lateralize to the side opposite the palsy.
Otologic examination
An otologic examination includes pneumatic otoscopy and tuning fork examination. An otologic cause should be considered if the history or physical examination demonstrates evidence of acute or chronic otitis media, including a tympanic membrane perforation, otorrhea, cholesteatoma, or granulation tissue, or if a history of ear surgery is noted. Concurrent rash or vesicles along the ear canal, pinna, and mouth should raise the suspicion for Ramsay Hunt syndrome (herpes zoster oticus).
The external auditory canal must be inspected for vesicles, injection or erythema, infection, or trauma. The patient may have decreased sensation to pinprick in the posterior auricular area. Tympanic membranes should be normal; the presence of inflammation, vesicles, or other signs of infection raises the possibility of complicated otitis media.
The patient who has paralysis of the stapedius muscle will report hyperacusis. This can be tested clinically using the stethoscope loudness test. In this, the patient wears a stethoscope, and an activated tuning fork is placed at its bell. The loud sound will lateralize to the side of the paralyzed stapedius muscle.
Ocular examination
With weakness/paralysis of the orbicularis oculi muscle (facial nerve innervation) and normal function of the levator muscle (oculomotor nerve innervation) and Mueller muscle (sympathetic innervation), the patient frequently is not able to close the eye completely on the affected side. On attempted eye closure, the eye rolls upward and inward on the affected side. (This is known as Bell phenomenon and is considered a normal response to eye closure.) In addition, the tear reflex is absent in many cases of Bell palsy.
For these reasons, the patient may have decreased tearing and susceptibility to corneal abrasion and dryness of the eye. The patient may appear to have loss of corneal reflex on the affected side; however, the contralateral eye blinks when testing the corneal reflex on the affected side.
Oral examination
A careful oral examination must be performed. Taste and salivation are affected in many patients with Bell palsy. Taste may be assessed by holding the tongue with gauze and testing each side of the tongue independently with salt, sugar, and vinegar. The mouth must be washed after testing with different substances. The affected side has decreased taste compared with the normal side.
Neurologic examination
Careful neurologic examination is necessary in patients with facial paralysis. This includes complete examination of all of the cranial nerves, sensory and motor testing, and cerebellar testing. A neurologic abnormality warrants neurologic referral and further testing, such as MRI of the brain, lumbar puncture, and EMG where appropriate.
Grading
The grading system developed by House and Brackmann categorizes Bell palsy on a scale of I to VI. Grade I is normal facial function.
Grade II is mild dysfunction. Characteristics include the following:
- Slight weakness is noted on close inspection
- Slight synkinesis may be present
- Normal symmetry and tone are noted at rest
- Forehead motion is moderate to good
- Complete eye closure is achieved with minimal effort
- Slight mouth asymmetry is noted
Grade III is moderate dysfunction. The following characteristics are found:
- An obvious, but not disfiguring, difference is noted between the 2 sides
- A noticeable, but not severe, synkinesis, contracture, or hemifacial spasm is present
- Normal symmetry and tone are noted at rest
- Forehead movement is slight to moderate
- Complete eye closure is achieved with effort
- A slightly weak mouth movement is noted with maximal effort
Grade IV is moderately severe dysfunction. Signs include the following:
- An obvious weakness and/or disfiguring asymmetry is noted
- Symmetry and tone are normal at rest
- No forehead motion is observed
- Eye closure is incomplete
- An asymmetrical mouth is noted with maximal effort
Grade V is severe dysfunction. Characteristics include the following:
- Only a barely perceptible motion is noted
- Asymmetry is noted at rest
- No forehead motion is observed
- Eye closure is incomplete
- Mouth movement is only slight.
Grade VI is total paralysis. The following are noted:
- Gross asymmetry
- No movement
In this system, grades I and II are considered good outcomes, grades III and IV represent moderate dysfunction, and grades V and VI describe poor results. Grade VI is defined as complete facial paralysis; all of the other grades are defined as incomplete. An incomplete facial paralysis denotes an anatomically and, to some degree, functionally intact nerve. The degree of facial nerve function should be noted in the chart at the patient’s initial visit.
In many cases, the history and physical examination of the patient establish the diagnosis of Bell palsy. If the clinical findings are doubtful or if paralysis lasts longer than 6-8 weeks, further investigations should be considered.
No specific diagnostic tests are available for Bell palsy, though the following may be useful for identifying or excluding other disorders:
- Rapid plasma reagin (RPR) and/or venereal disease research laboratory (VDRL) test or fluorescent treponemal antibody absorption (FTA-ABS) test
- HIV screening by means of enzyme-linked immunosorbent assay (ELISA) and/or Western blot
- Complete blood cell (CBC) count
- Erythrocyte sedimentation rate measurement
- Thyroid function studies
- Serum glucose level
- Cerebrospinal fluid analysis
In addition to the above tests, blood glucose or hemoglobin A1c levels may be obtained to determine if the patient has undiagnosed diabetes. Persons with diabetes have a 29% higher risk of being affected by Bell palsy than do persons without diabetes.
Serum titers for herpes simplex virus (HSV) may be obtained. However, this test is usually not helpful, owing to the ubiquitous nature of this virus.
Antineutrophil cytoplasmic antibody (cANCA) levels are indicated, if applicable, to exclude Wegener granulomatosis. In areas where Lyme disease is endemic, serum titers (immunoglobulin M [IgM] and IgG) for Borrelia burgdorferi should be obtained.
Serum titers (IgM and IgA) for Mycoplasma pneumoniae may be obtained. A study in Germany measured titers in patients with Bell palsy and found that several patients had elevated titers for M pneumoniae, though only 2 of those who tested positive had respiratory symptoms.
Salivary flow test
Salivary flow also may be tested. The physician places a small catheter into the paralyzed and normal submandibular glands. The patient is then asked to suck on a lemon, and the salivary flow is compared between the 2 sides. The normal side is the control.
Schirmer blotting test
The Schirmer blotting test may be used to assess tearing function. The use of benzene will stimulate the nasolacrimal reflex, and the degree of tearing can be compared between the paralyzed and normal sides.
Nerve excitability test
The nerve excitability test determines the threshold of the electrical stimulus needed to produce visible muscle twitching. This test is technically challenging and has very limited clinical availability.
Imaging considerations
If the history and physical examination lead to a diagnosis of Bell palsy, then immediate imaging is not necessary, because most patients with Bell palsy improve within 8-10 weeks. If the paralysis does not improve or worsens, imaging may be useful. If the patient has a palpable parotid mass, imaging may be necessary.
CT Scanning and MRI
Imaging with CT scanning or other methods is indicated if there are other associated physical findings or if the paresis is progressive and unremitting. CT scanning demonstrates the architecture of the temporal bone and may be used if some other pathology is suspected.
MRI is useful as a means of excluding other pathologies as the cause of paralysis and is preferred for imaging the cerebellopontine angle.
MRI in patients with Bell palsy may show enhancement of the seventh cranial nerve (facial nerve) at or near the geniculate ganglion. Alternatively, MRI may demonstrate a neoplasm compressing the facial nerve. Tumors that compress or involve the facial nerve include schwannoma (most common), hemangioma, meningioma, and sclerosing hemangioma.
Perform gadolinium-enhanced MRI when findings are atypical or when the facial nerve paralysis appears central, to rule out a tumor or vascular compression. Increased signal intensity of the premeatal or intratemporal segment of the facial nerve after administration of gadolinium has been noted in patients with Bell palsy. Attempts to correlate outcome with quantification of signal intensity increases have yielded contradictory results.
Conduction Testing and EMG
Useful tests for evaluation of the function of the facial nerve include nerve conduction testing and EMG. Nerve conduction velocities and EMG produce a graphic readout of the electrical currents, displayed by stimulating the facial nerve and recording the excitability of the facial muscles it supplies. These tests may aid in assessing the outcome of a patient who has persistent and severe Bell palsy.
This testing is not part of the acute workup; the tests are most useful when performed 3-10 days after the onset of paralysis. Note that most electromyographic/nerve conduction studies do not show an abnormality for 3 weeks following a peripheral nerve injury.
Comparison to the contralateral side helps to demonstrate the extent of nerve injury and has prognostic implications. Nerve conduction responses are abnormal if a difference of 50% in amplitude between the paralyzed and normal side is detected; a difference of 90% between the 2 sides suggests a poorer prognosis.
May et al demonstrated that prognosis may be favorable if the motor amplitude of the affected side is greater than 25% of that of the normal side. An incomplete recovery was observed in patients whose results demonstrated less than 25% amplitude on the paralyzed side. Blink reflexes can be used to measure conduction across the involved segment, but they are commonly absent in Bell palsy.
Electroneurography
Electroneurography is a physiologic test that uses EMG to objectively measure the difference between potentials generated by the facial musculature on both sides of the face in response to a supramaximal electrical stimulation of the facial nerve. Because all electrodiagnostic testing is performed on the nerve distal to the proposed site of injury, sufficient time is needed for wallerian degeneration to occur, usually 48-72 hours. Testing should begin 3 days from the onset of complete paralysis.
Electrodiagnostic testing measures the facial nerve degeneration indirectly. If a patient does not reach 90% degeneration within the first 3 weeks of the onset of paralysis, some studies suggest that the prognosis is excellent, with over 80-100% of the patients recovering with excellent function.
The patients who reach over 90% degeneration within the first 3 weeks of the onset of paralysis have a much more guarded prognosis, with only 50% having good recovery of facial motion. The rate of degeneration also predicts the prognosis. Patients who have 90% degeneration by 5 days have a worse prognosis than those with 90% degeneration at 14 days.
Brainstem Auditory Evoked Response and Audiometry
Brainstem auditory evoked response (BAER) may be obtained in patients with peripheral facial nerve lesions and other neurologic involvement. This test measures the transmission of response through the brainstem and is effective in detecting, notably, retrocochlear lesions.
Hendrix and Melnick evaluated the BAER of 17 patients with Bell palsy and found no evidence of retrocochlear lesions of the auditory system in any of the patients. In study by Shannon et al, BAER was recorded in 27 patients with Bell palsy; only 6 patients had prolonged brainstem transmission but normal auditory function.
These studies were small and do not support routine use of BAER in patients with Bell palsy. However, when a patient presents with multiple cranial neuropathies (eg, of the seventh and eighth cranial nerves), BAER may be useful.
If hearing loss is suspected, audiography and auditory evoked potentials (AEPs) should be pursued once an underlying structural lesion has been excluded. Typically, the hearing threshold is not affected by Bell palsy. Impedance testing may reveal an absent or diminished stapedial reflex because of paresis of the stapedial branch of the facial nerve.
Blepharokymographic Analysis
Blepharokymographic analysis, a high-speed eyelid motion-analysis system, has been used to evaluate movement of the eyelids. Computer-based analysis may prove helpful in diagnosing Bell palsy, predicting prognosis, and evaluating response to therapeutic measures such as placement of a gold weight in the affected upper eyelid (used in cases in which spontaneous recovery has been limited).
Histologic Findings
In a review of 12 autopsy cases of patients with Bell palsy, most cases showed inflammatory changes around the mastoid cells and walls of the arteries. The most common site of involvement was the geniculate ganglion. Surgical findings described constriction of the nerve at the stylomastoid foramen, with swelling of the nerve itself. Microscopic findings showed an inflammatory reaction with infiltration of macrophages on the nerve.
Treatment and Management
Because persons with true Bell palsy generally have an excellent prognosis, and because spontaneous recovery is fairly common, treatment of Bell palsy is still controversial. The goals of treatment are to improve facial nerve (seventh cranial nerve) function and reduce neuronal damage.
Many issues must be addressed in treating patients with Bell palsy. The most important is the onset of symptoms. Treatment may be considered for patients who present within 1-4 days of the onset of paralysis.
Patients with Bell palsy frequently present to the emergency department (ED). The role of the ED clinician consists of the following:
- Initiate appropriate treatment
- Protect the eye
- Arrange appropriate medical follow-up care
The American Academy of Neurology (AAN) published a practice parameter in 2001 stating that steroids are probably effective and acyclovir (with prednisone) is possibly effective for the treatment of Bell palsy. There was insufficient evidence for recommendations on facial decompression surgery.
In 2012, the AAN released guidelines stating that steroids are highly likely to be effective and increase the likelihood of recovery of facial nerve function in new-onset Bell palsy
A variety of nonpharmacologic measures have been used to treat Bell palsy, including physical therapy (eg, facial exercises, neuromuscular retraining ) and acupuncture. No adverse effects of these treatments have been reported. Reviews suggest that physical therapy may result in faster recovery and reduced sequelae, but further randomized, controlled trials are needed to confirm any benefit.
Surgical options
Surgical options for Bell palsy include the following:
- Facial nerve decompression
- Subocularis oculi fat (SOOF) lift
- Implantable devices (eg, gold weights) placed into the eyelid
- Tarsorrhaphy
- Transposition of the temporalis muscle
- Facial nerve grafting
- Direct brow lift
Anecdotal evidence suggests that surgical repair by using a combination of procedures tailored to the patients’ clinical findings works well for improving symptoms and exposure. Most patients who have had severe corneal exposure from lagophthalmos with or without paralytic ectropion have received a combination of lateral tarsal strip placement, SOOF lift, and gold-weight implantation. Patients without severe exposure have received a single procedure or combinations of procedures.
Pharmacologic Therapy
The most widely accepted treatment for Bell palsy is corticosteroid therapy. However, the use of steroids is still controversial because most patients recover without treatment. Antiviral agents have also been studied in this setting, as have combinations of the 2 types of drugs.
Corticosteroids
As previously mentioned, 2012 guidelines from the AAN state that steroids are highly likely to be effective and increase the likelihood of recovery of facial nerve function in new-onset Bell palsy
Guidelines from the American Academy of Otolaryngology–Head and Neck Surgery Foundation (AAO-HNSF) were issued in November 2013 that also support the AAN guidelines. The guidelines recommend use of corticosteroids within 72 hours from the onset of symptoms. Antiviral agents (eg, acyclovir, valacyclovir) may be considered if a viral etiology is suspected, but only in combination with corticosteroids.
Many trials have been carried out to study the efficacy of prednisone in Bell palsy. In 1972, for example, Adour et al conducted a large, controlled clinical trial that found that 89% of patients treated with prednisone had full recovery, compared with 64% of patients treated with placebo.
This trial and other early studies, however, showed conflicting results for steroid use in treating Bell palsy, and they were limited in their size.
However, 3 subsequent randomized, controlled trials showed significant improvement in outcomes when prednisolone was started within 72 hours of symptom onset. Based on these 3 studies, steroids should be strongly considered to optimize outcomes. Once the decision to use steroids is made, the consensus is that this treatment should be started immediately.
One of the 3 studies—a double-blind, randomized trial from Scotland involving 551 patients with Bell palsy who were recruited within 72 hours of symptom onset—demonstrated that early treatment with prednisolone can significantly improve the chances of complete recovery at 3 and 9 months. In contrast, acyclovir given alone did not show any significant difference in the rate of facial recovery compared with placebo, and there was no additional benefit from combining acyclovir and prednisolone compared with prednisolone alone.
A larger double-blind, controlled trial showed that prednisolone significantly shortened the time to complete recovery, while valacyclovir did not affect facial recovery compared with placebo. Further analysis showed that patients treated with prednisolone within 48 hours had significantly higher rates of complete recovery than did those who were not treated, whereas no significant difference in recovery rate was seen between patients treated at 49-72 hours and untreated patients.
The recommended dose of prednisone for the treatment of Bell palsy is 1 mg/kg or 60 mg/day for 6 days, followed by a taper, for a total of 10 days. Caution should be used in patients with any of the following:
- Tuberculosis
- Immunocompromise
- Pregnancy
- Active infection
- Sarcoidosis
- Sepsis
- Peptic ulcer disease
- Diabetes mellitus
- Renal or hepatic dysfunction
- Malignant hypertension
High-dose steroids (>120 mg/day of prednisone) have been safely used to treat Bell palsy in patients with diabetes ; however, optimal dosing has not been established. Caution should be used in these cases because of the risk of hyperglycemia.
Antiviral agents
Evaluation of the use of antiviral medicines in Bell palsy has shown limited benefit from these drugs, with 3 randomized, controlled trials having demonstrated no benefit from them. However, given the evidence suggesting that a large percentage of Bell palsy cases may result from a viral infection, the use of antiviral agents may be reasonable in certain situations.
The 2001 AAN practice perameter suggested that the use of acyclovir for the treatment of Bell palsy is only possibly effective and that therapy with this agent alone is not effective in facial recovery. According to the academy's 2012 guidelines, benefit from antivirals has not been established and, at best, is likely to be modest.
The Scottish study cited earlier suggested that prednisolone, and not acyclovir, is useful for facial recovery in Bell palsy.
A Cochrane review found no significant benefit to the use of antivirals over placebo in reducing the rate of incomplete recovery from Bell palsy. This meta-analysis looked at 7 studies involving a total of 1987 patients treated between 1966 and 2008.
Acyclovir (Zovirax) is administered at a dosage of 400 mg orally 5 times daily for 10 days. Evidence supports HSV as a major cause of Bell palsy; if varicella zoster virus (VZV) is suspected, higher doses may be needed (800 mg orally 5 times daily).
Valacyclovir (Valtrex), taken orally in doses of 500 mg twice daily for 5 days, may be used instead of acyclovir. Although it is more expensive, it may be associated with better compliance. If VZV is the cause of Bell palsy, higher doses may be needed (1000 mg orally 3 times daily). Because of the increased cost and greater risk of side effects with higher doses, however, valacyclovir cannot be routinely recommended for the treatment of Bell palsy at this time.
Corticosteroid-antiviral combinations
A prospective randomized trial with 101 patients comparing prednisone with acyclovir demonstrated that the prednisone group had better clinical recovery. In another prospective, randomized trial, with 99 patients, the combination of prednisone and acyclovir was more effective than prednisone monotherapy in preventing nerve degeneration, as measured by electrodiagnostic tests.
A Japanese randomized, prospective study of 221 patients with Bell palsy showed significant improvement in facial function using a combination of prednisone and valacyclovir therapy versus using prednisone alone. This improvement was noted in patients who had severe to complete facial palsy.
Quant et al conducted a meta-analysis of published studies from 1984 to January 2009 that showed no improved benefit (with respect to degree of facial muscle recovery in patients with Bell palsy) from the use of corticosteroids plus antiviral agents as compared with corticosteroid therapy alone. Six trials (representing pooled data from 1145 patients) were examined and included 574 patients who received corticosteroids alone and 571 patients who received corticosteroids and antiviral agents.
Quant et al suggest that the routine use of antiviral agents is not warranted; however, future studies should improve diagnostic efforts to identify herpes virus as a potential etiology. Additionally, newer antiviral agents may prove more beneficial than older antiviral agents used in the studies analyzed to date.
Contrary to the meta-analyses by Quant et al and Cochrane, de Almeida and colleagues found that antiviral agents, when combined with corticosteroids, were associated with greater risk reduction of borderline significance than were corticosteroids alone. Their meta-analysis examined 18 trials involving a total of 2786 patients.
If antiviral agents are used, they should be initiated in conjunction with corticosteroids. Future studies will be needed to determine which population will most benefit from antiviral therapy.
Local Treatment
It is universally accepted that eye care is imperative in Bell palsy. The patient’s eye is at risk for drying, corneal abrasion, and corneal ulcers.
In most cases, topical ocular lubrication (with artificial tears during the day and lubricating ophthalmic ointment at night, or occasionally ointment day and night) is sufficient to prevent the complications of corneal exposure. Punctal plugs may be helpful if dryness of the cornea is a persistent problem.
Occluding the eyelids by using tape or by applying a patch for 1 or 2 days may help to heal corneal erosions. Care must be taken to prevent worsening the abrasion with the tape or patch by ensuring that the eyelid is securely closed. Clear plastic wrap, cut to 8 X 10 cm and applied with generous amounts of ointment as a nighttime occlusive bandage, may be required.
External eyelid weights are available to improve mechanical blink. The weights are attached to the upper lid with an adhesive and are available in different skin tones.
Lower-lid ectropion or droop can temporarily be helped by applying tape below the lid margin in the center of the lower lid; the lid is pulled laterally and upward to anchor on the orbital rim.
Botulinum toxin can be injected transcutaneously or subconjunctivally at the upper border of the tarsus and aimed at the levator muscle to produce complete ptosis and to protect the cornea. Botulinum toxin may help in relaxing the facial muscles after they have developed mass contraction, though the results are not as satisfying in patients with Bell palsy as in patients with idiopathic hemifacial spasm.
Facial Nerve Decompression
Surgery to decompress the facial nerve is controversial. Patients with a poor prognosis, identified by facial nerve testing or persistent paralysis, appear to benefit the most from surgical intervention. However, studies have been mixed as far as benefit from surgery.
Surgery may be considered in patients with complete Bell palsy that has not responded to medical therapy and with greater than 90% axonal degeneration, as shown on facial nerve EMG within 3 weeks of the onset of paralysis. The problem must be localized with MRI. The surgeon can then decide if the maxillary segment should be decompressed externally or if the labyrinthine segment and geniculate ganglion should be decompressed with a middle fossa craniotomy.
A study in patients with greater than 90% degeneration demonstrated superior results in the cohort that underwent middle fossa decompression, compared with the cohort that chose not to pursue surgical decompression. In the surgical group, 91% of cases exhibited a postoperative House-Brackmann grade of I or II. In the nonsurgical group, 58% of the patients had a poor result, with a House-Brackmann grade of III or IV at 7 months. The best surgical results were obtained when the procedure was done within 14 days after the onset of paralysis.
Subocularis Oculi Fat Lift
The SOOF is deep to the orbicularis oculi muscle and superficial to the periosteum below the inferior orbital rim. An SOOF lift is designed to lift and suspend the midfacial musculature. The procedure may also elevate the upper lip and the angle of the mouth to improve facial symmetry.
Lateral tarsal strip procedure
An SOOF lift is commonly performed in conjunction with a lateral tarsal strip procedure to correct horizontal lower-lid laxity and to improve apposition of the lid to the globe. First, lateral canthotomy and cantholysis is performed. Then, the anterior lamella is removed, and the lateral tarsal strip is shortened and attached to the periosteum at the lateral orbital rim.
Implants in Eyelid
Implantable devices have been used to restore dynamic lid closure in cases of severe, symptomatic lagophthalmos. These procedures are best for patients with poor Bell phenomenon and decreased corneal sensation. Gold or platinum weights, a weight-adjustable magnet, or palpebral springs can be inserted into the eyelids. Pretarsal gold-weight implantation is most commonly performed.
The implants are inert and composed of 99.99% pure gold or platinum. Sizes range from 0.6-1.8 g. The weight allows the upper eyelid to close with gravity when the levator palpebrae are relaxed. Therefore, patients must sleep with their head slightly elevated.
The implants are easily removed if nerve function returns. Complications include migration of the implant, inflammation, allergic reaction, and extrusion.
Tarsorrhaphy
Tarsorrhaphy decreases horizontal lid opening by fusing the eyelid margins together, increasing support of the precorneal lake of tears and improving coverage of the eye during sleep. The procedure can be done in the office and is particularly suitable for patients who are unable or unwilling to undergo other surgery. It can be completed as either a temporary or a permanent measure. Permanent tarsorrhaphy is performed if nerve recovery is not expected.
Tarsorrhaphy can be performed laterally, centrally, or medially. The lateral procedure is the most common; however, it can restrict the monocular temporal visual field. Central tarsorrhaphy offers good corneal protection, but it occludes vision and can be cosmetically unacceptable. Medial or paracentral tarsorrhaphy is performed lateral to the lacrimal puncta and can offer good lid closure without substantially affecting the visual field.
Muscle Transposition, Nerve Grafting, and Brow Lift
Transposition of temporalis
Transposition of the temporalis muscle can be used to reanimate the face and to provide lid closure by using the fifth cranial nerve. Strips from the muscle and fascia are placed in the upper and lower lids as an encircling sling. Patients initiate movement by chewing or clenching their teeth.
Facial nerve grafting or hypoglossal-facial nerve anastomosis
Reinnervation of the facial nerve by means of facial nerve grafting or hypoglossal-facial nerve anastomosis can be used in cases of clinically significant permanent paralysis to help restore relatively normal function to the orbicularis oculi muscle or eyelids.
Direct brow lift
Brow ptosis is repaired with a direct brow lift. Care should be taken in the presence of corneal decompensation because lifting the brow can cause worsening of lagophthalmos, especially if lid closure is poor. A gold-weight implant can be placed or lower-lid resuspension can be performed simultaneously to prevent this complication.
Consultations and Monitoring
Consultations
If the patient’s paralysis is not resolving or is progressing to complete paralysis, a thorough neurologic assessment and an examination of the head, eyes, ears, nose, and throat should be performed to rule out neoplastic causes of facial nerve palsy.
If the initial diagnostic impression based on the history and physical examination of the patient is not Bell palsy, then consultation with a neurologist or otolaryngologist is needed. For example, consultation with an otolaryngologist should be made for the patient who has facial palsy and pain and in whom the ear, nose, and throat examination does not show auricular vesicles (as in Ramsay Hunt syndrome). These patients should be evaluated for malignancy or other structural lesions of the facial nerve.
Consultation with a neurologist or otolaryngologist should also be sought if the paralysis persists for several months.
An evaluation by an otolaryngologist may be indicated for patients with a prolonged course, for the consideration of surgical decompression of the facial nerve. Patients who report persistent dry eye or painful eye should be referred to an ophthalmologist. An evaluation by a specialist in infectious disease may be indicated if results of laboratory studies are positive for Lyme disease, syphilis, or HIV infection.
Monitoring
The patient should be monitored if the initial EMG shows that the function of the involved facial muscles is less than 25% of the normal side’s facial muscle function. If the residual paralysis is severe, the patient should be referred for counseling.
Medication Summary
The goals of pharmacotherapy are to reduce morbidity and prevent complications. Agents used in cases of Bell palsy include corticosteroids and antiviral agents. Early treatment with corticosteroids is the most widely accepted treatment, but it remains controversial because most patients recover without treatment. The literature offers less support for the use of antiviral agents in either monotherapy or combination therapy, although treatment with combinations of corticosteroids and antiviral agents is somewhat better supported.
Corticosteroids
Class Summary
Prednisone can be used in the treatment of Bell palsy but has many adverse effects, including the following:
- Fluid retention
- Hypokalemia
- Myopathy
- Peptic ulcer
- Headache (pseudotumor)
- Menstrual irregularities
- Cataracts
- Glaucoma
- Manifestation of latent diabetes mellitus
In addition, signs of infection may be masked in patients taking prednisone. Physicians should use caution when using prednisone in patients with the aforementioned conditions.
Antivirals
Class Summary
Acyclovir and valacyclovir have been administered in the treatment of Bell palsy in combination with prednisone or have been used alone in patients who cannot take prednisone. The use of antivirals has proved most beneficial in patients with severe to complete facial palsy
 Posted in
Posted in
Facial paralysis can be temporary or enduring. After approximately six months, most Bell’s palsy patients, for example, will get better absolutely. Stroke victims and trauma victims, though, often have to undergo Treatment for Bell's Palsy for months or even years.
ReplyDeleteGinger is one of the most used Herbal Remedy for Bell’s Palsy Herbal Treatment in India as part of their cuisine. It has anti-inflammatory properties which are decreasing the symptoms caused by Bell’s palsy.
ReplyDeleteI started on COPD Herbal treatment from Ultimate Health Home, the treatment worked incredibly for my lungs condition. I used the herbal treatment for almost 4 months, it reversed my COPD. My severe shortness of breath, dry cough, chest tightness gradually disappeared. Reach Ultimate Health Home via their email at ultimatehealthhome@gmail.com . I can breath much better and It feels comfortable!
ReplyDelete